

Hemodynamically unstable non-compressible penetrating torso trauma: a practical surgical approach
- PMID: 34188320
- PMCID: PMC8216055
- DOI: 10.25100/cm.v52i2.4592
Hemodynamically unstable non-compressible penetrating torso trauma: a practical surgical approach
Abstract
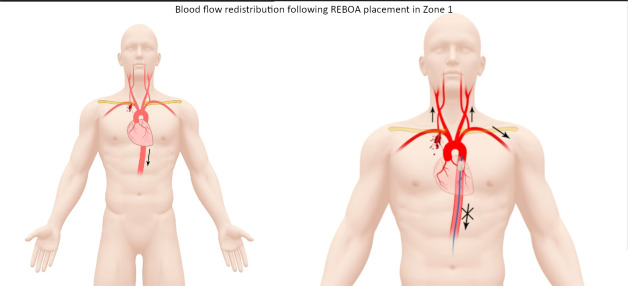
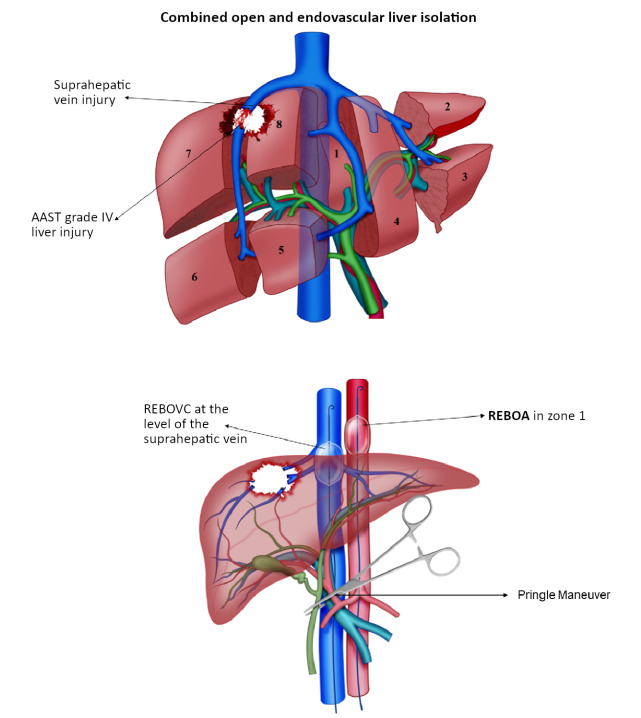
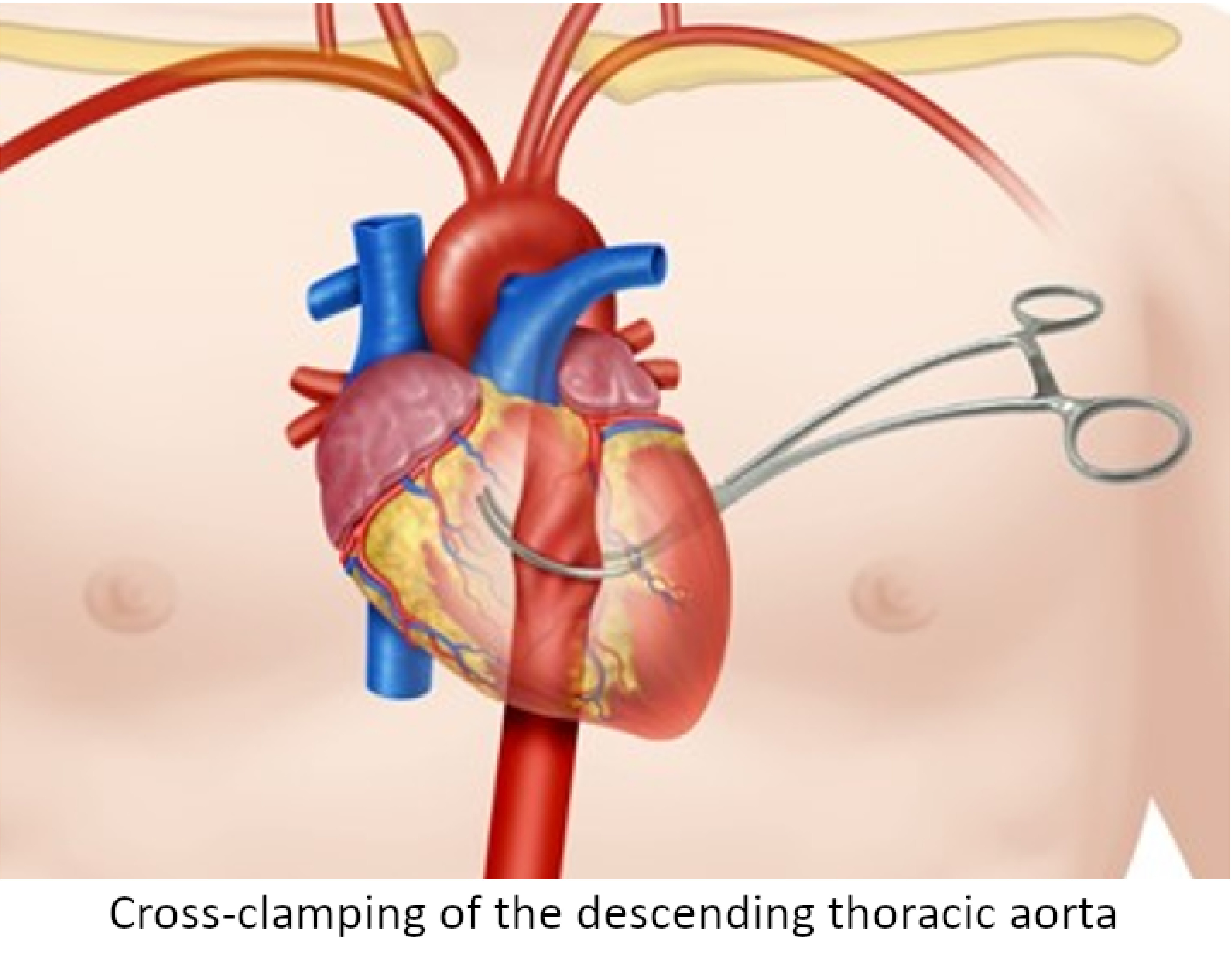
Penetrating torso trauma is the second leading cause of death following head injury. Traffic accidents, falls and overall blunt trauma are the most common mechanism of injuries in developed countries; whereas, penetrating trauma which includes gunshot and stabs wounds is more prevalent in developing countries due to ongoing violence and social unrest. Penetrating chest and abdominal trauma have high mortality rates at the scene of the incident when important structures such as the heart, great vessels, or liver are involved. Current controversies surround the optimal surgical approach of these cases including the use of an endovascular device such as the Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) and the timing of additional imaging aids. This article aims to shed light on this subject based on the experience earned during the past 30 years in trauma critical care management of the severely injured patient. We have found that prioritizing the fact that the patient is hemodynamically unstable and obtaining early open or endovascular occlusion of the aorta to gain ground on avoiding the development of the lethal diamond is of utmost importance. Damage control surgery starts with choosing the right surgery of the right cavity in the right patient. For this purpose, we present a practical and simple guide on how to perform the surgical approach to penetrating torso trauma in a hemodynamically unstable patient.
El trauma penetrante del torso representa la segunda causa de muerte de origen traumático después del trauma craneoencefálico. En países desarrollados existe mayor prevalencia de trauma cerrado, asociado principalmente a accidentes de tránsito o caídas de grandes alturas. Mientas, que en países en vía de desarrollo el trauma penetrante es más prevalente con heridas por arma de fuego o por arma blanca asociado a la violencia y las desigualdades sociales. El trauma penetrante torácico y abdominal pueden presentar altas tasas de mortalidad en la escena del trauma si se comprometen estructuras importantes como el corazón, los grandes vasos o el hígado. Actualmente, existen controversias sobre el adecuado abordaje quirúrgico con la implementación o no de dispositivos endovasculares como el balón de resucitación endovascular de oclusión aórtica (Resuscitative Endovascular Balloon Oclussion of the Aorta - REBOA) y la realización de ayudas imagenológicas. El objetivo de este artículo es presentar el conocimiento sobre este tema, basado en la experiencia adquirida durante los últimos 30 años con el manejo del trauma, cirugía general y cuidado crítico. Sostenemos que en un paciente hemodinámicamente inestable se debe realizar una temprana oclusión aórtica endovascular o abierta con el objetivo de evitar el desarrollo o propagación del rombo de la muerte. Con este propósito, presentamos una guía práctica y sencilla sobre el abordaje quirúrgico del paciente hemodinámicamente inestable con trauma penetrante del torso.
Keywords: Damage control surgery; REBOA; aortic occlusion; hemodynamically unstable non-compressible penetrating torso trauma; median sternotomy.
Copyright © 2021 Colombia Medica.
Conflict of interest statement
Conflicts of interest: The authors declare that they have no conflict of interest
Figures









References
-
- Ordoñez CA, Manzano-Nunez R, Naranjo MP, Foianini E, Cevallos C, Londoño MA. Casualties of peace An analysis of casualties admitted to the intensive care unit during the negotiation of the comprehensive Colombian process of peace. World J Emerg Surg. 2018;13:2–2. doi: 10.1186/s13017-017-0161-2. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
