

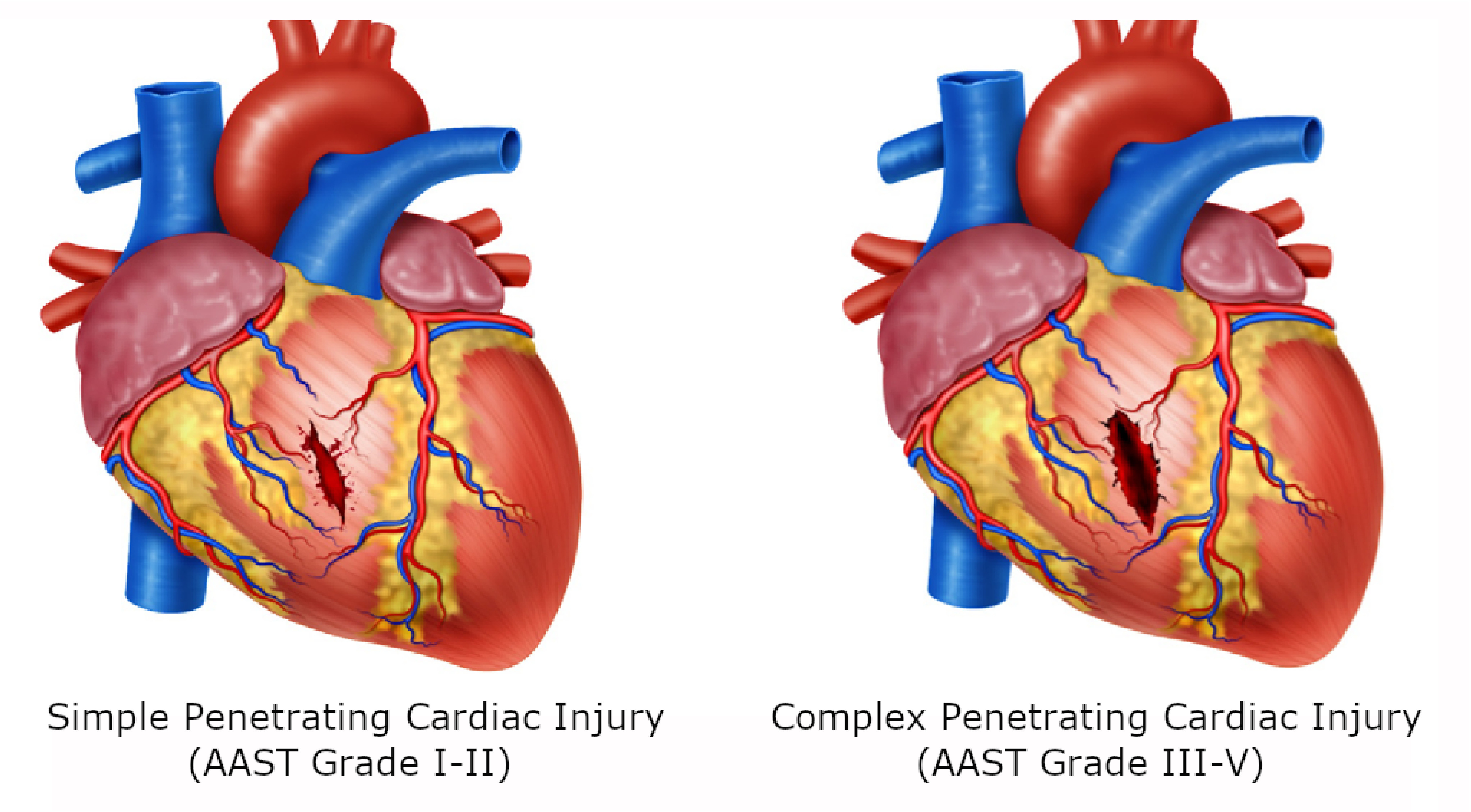
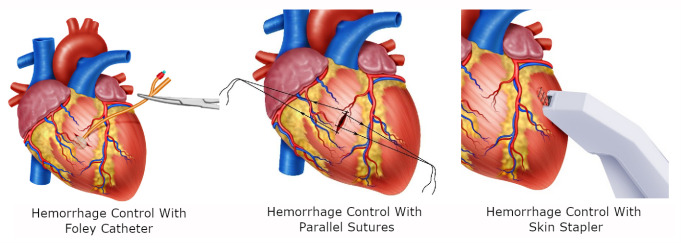
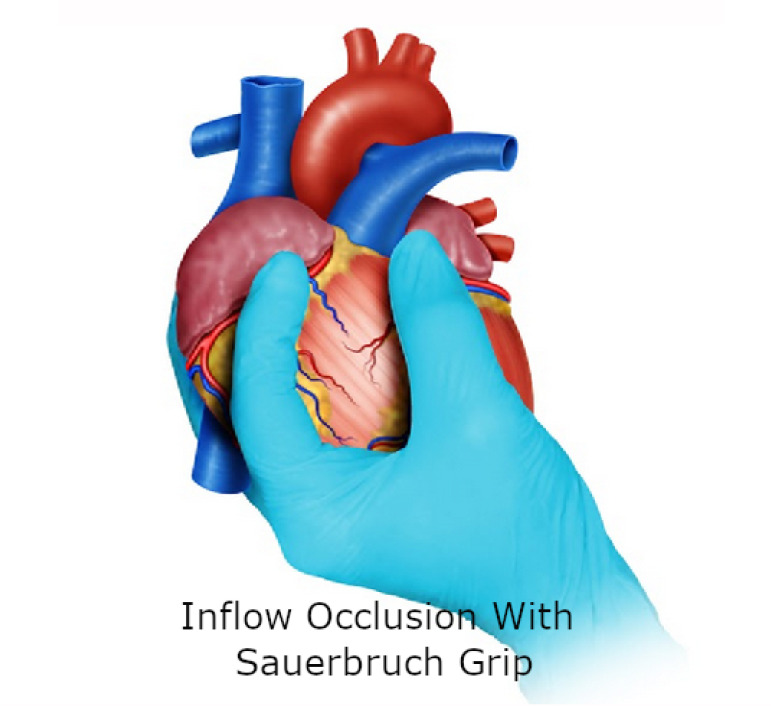
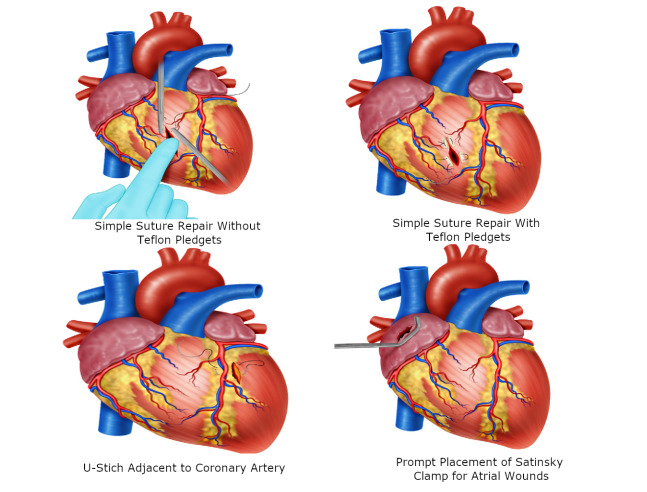
Damage control in penetrating cardiac trauma
- PMID: 34188321
- PMCID: PMC8216058
- DOI: 10.25100/cm.v52i2.4519
Damage control in penetrating cardiac trauma
Abstract
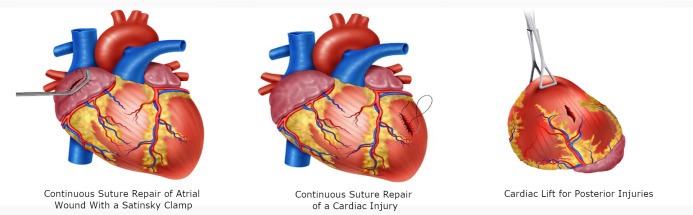
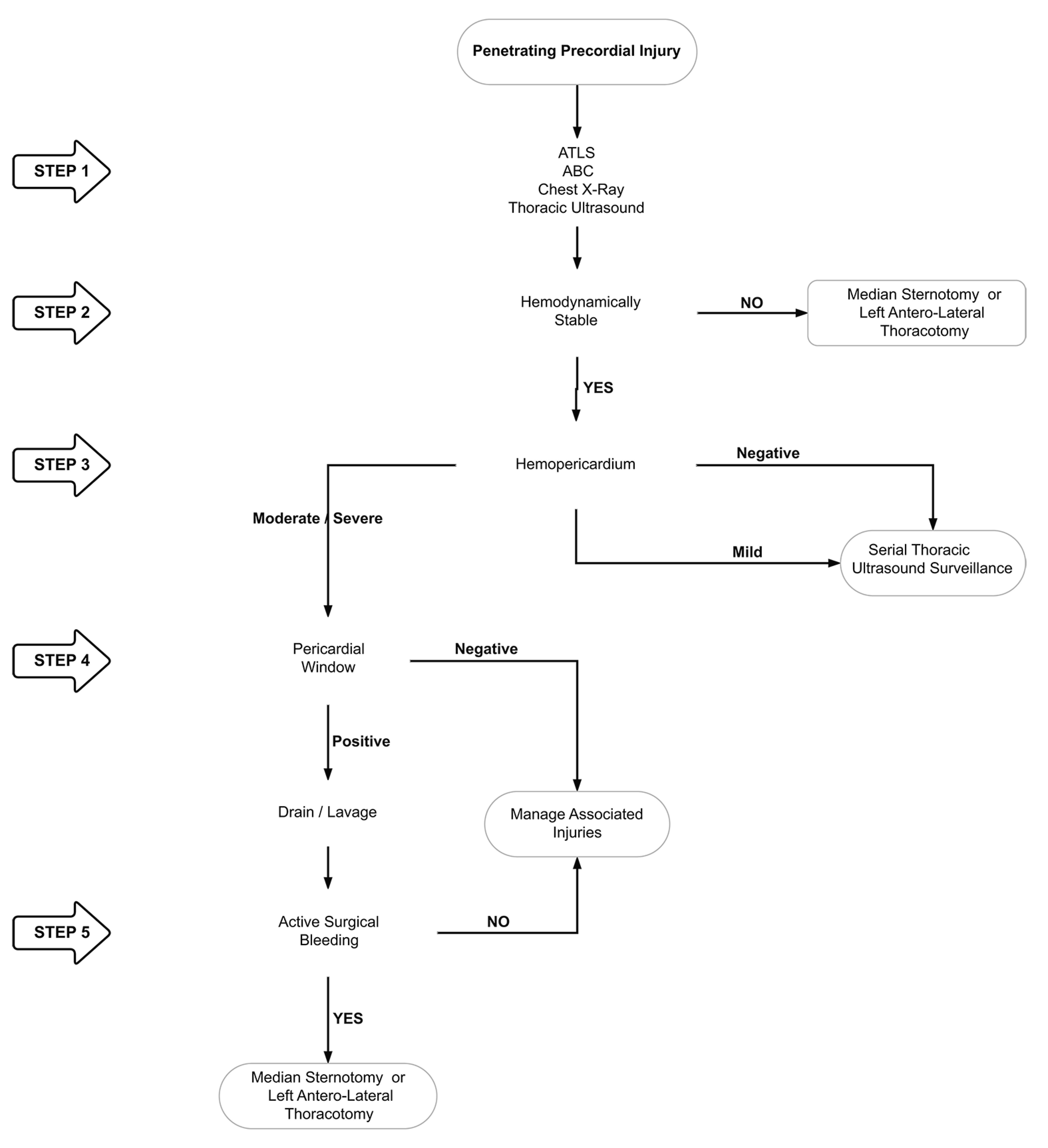
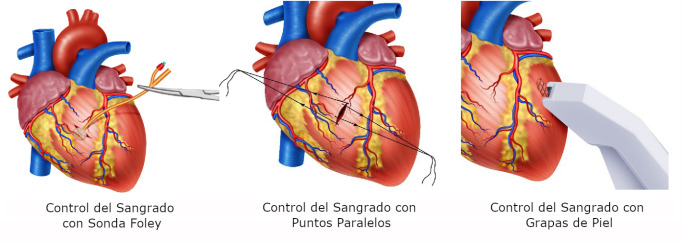
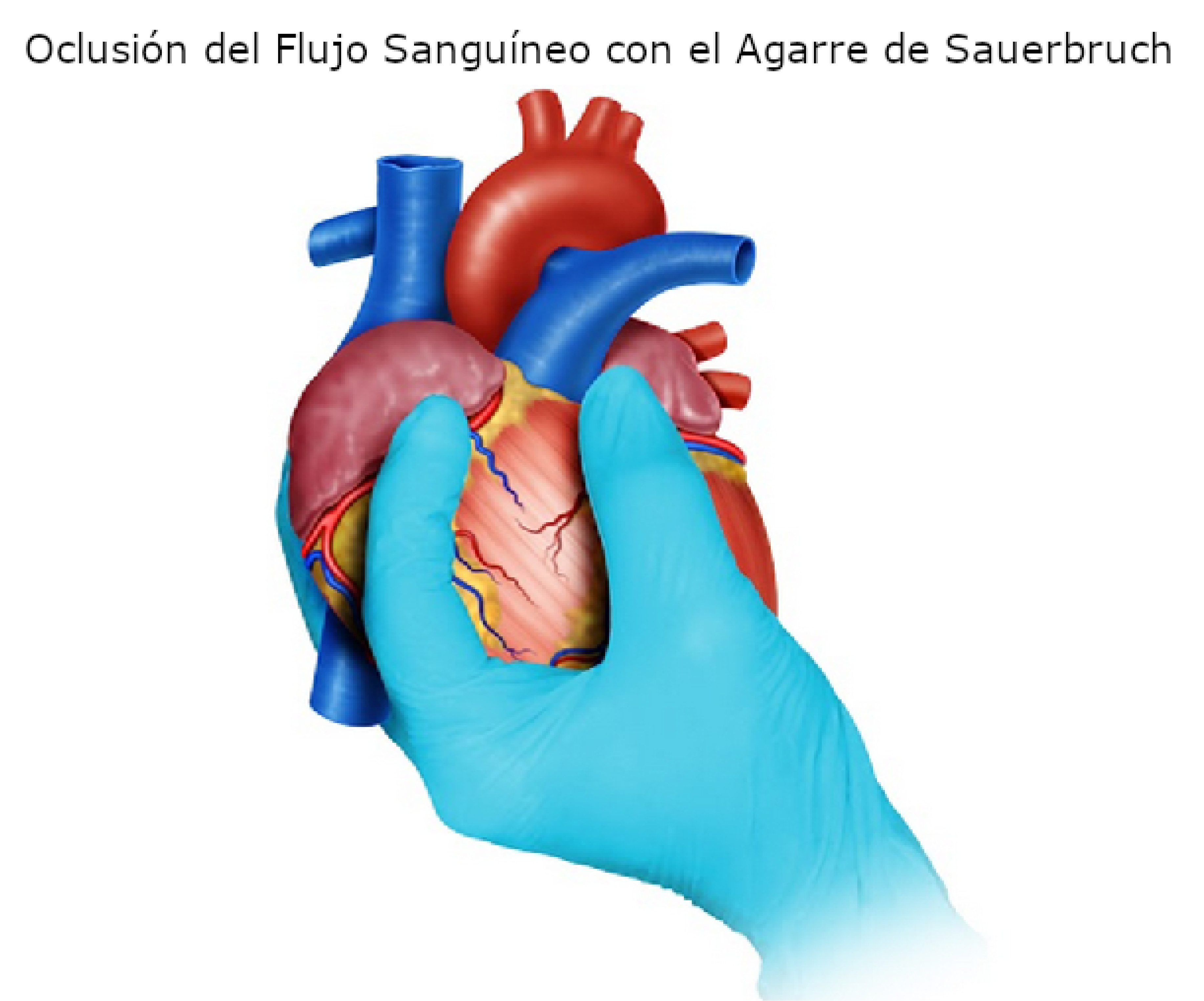
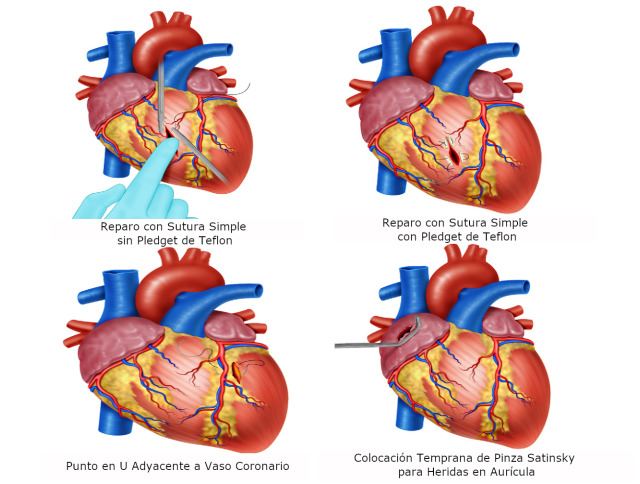
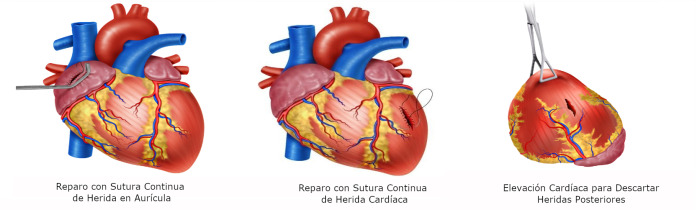
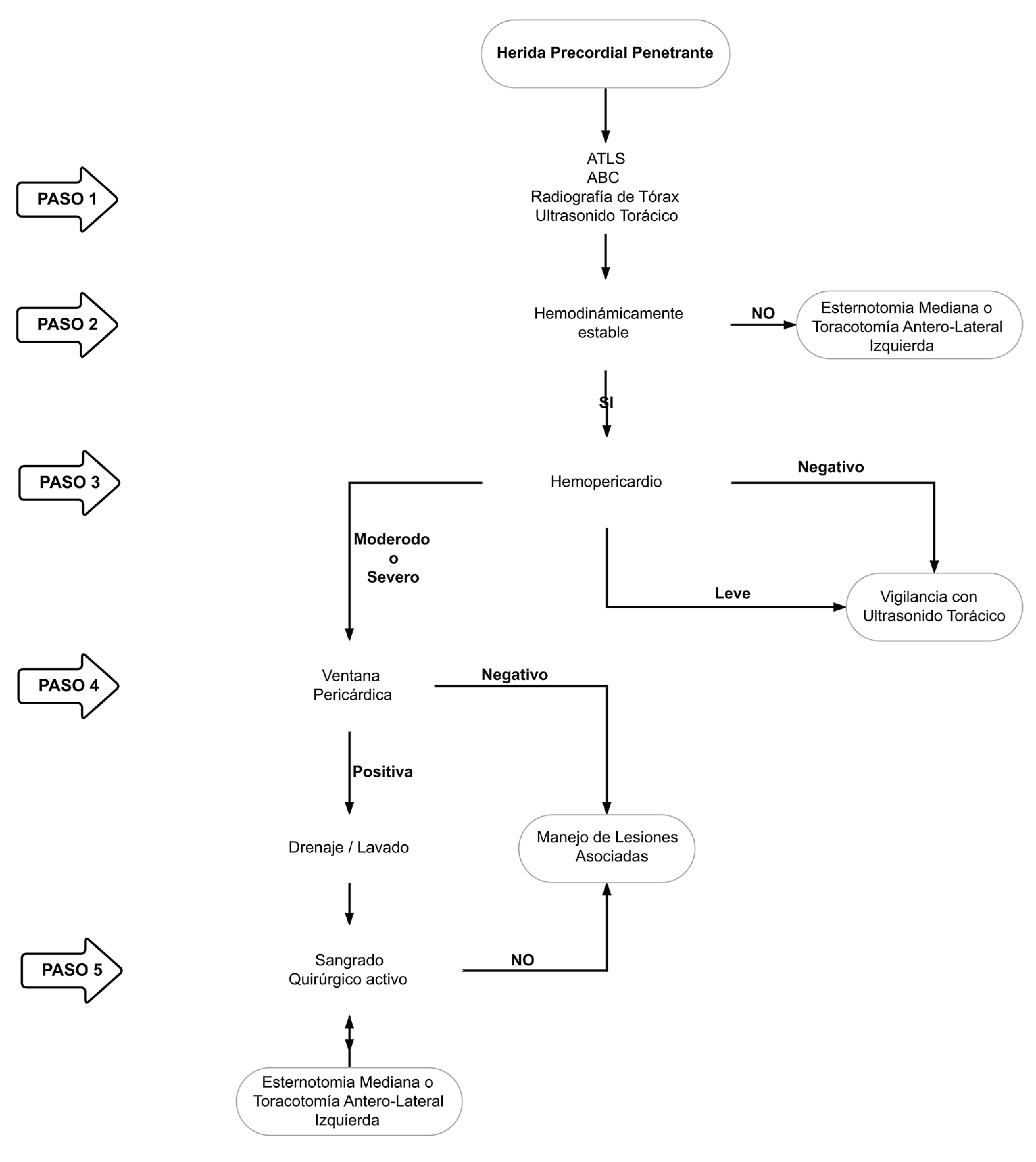
Definitive management of hemodynamically stable patients with penetrating cardiac injuries remains controversial between those who propose aggressive invasive care versus those who opt for a less invasive or non-operative approach. This controversy even extends to cases of hemodynamically unstable patients in which damage control surgery is thought to be useful and effective. The aim of this article is to delineate our experience in the surgical management of penetrating cardiac injuries via the creation of a clear and practical algorithm that includes basic principles of damage control surgery. We recommend that all patients with precordial penetrating injuries undergo trans-thoracic ultrasound screening as an integral component of their initial evaluation. In those patients who arrive hemodynamically stable but have a positive ultrasound, a pericardial window with lavage and drainage should follow. We want to emphasize the importance of the pericardial lavage and drainage in the surgical management algorithm of these patients. Before this concept, all positive pericardial windows ended up in an open chest exploration. With the coming of the pericardial lavage and drainage procedure, the reported literature and our experience have shown that 25% of positive pericardial windows do not benefit and/or require further invasive procedures. However, in hemodynamically unstable patients, damage control surgery may still be required to control ongoing bleeding. For this purpose, we propose a surgical management algorithm that includes all of these essential clinical aspects in the care of these patients.
El manejo definitivo de los pacientes hemodinámicamente estables con heridas cardíacas penetrantes continúa siendo controversial con abordajes invasivos versus manejos conservadores. Estas posiciones contrarias se extienden hasta aquellos casos de pacientes hemodinámicamente inestables donde se ha descrito y considerado la cirugía de control de daños como un procedimiento útil y efectivo. El objetivo de este artículo es presentar la experiencia en el manejo quirúrgico de heridas cardíacas penetrantes con la creación de un algoritmo práctico que incluye los principios básicos del control de daños. Se recomienda que a todos los pacientes con heridas precordiales penetrantes se les debe realizar un ultrasonido torácico como componente integral de la evaluación inicial. Aquellos que presenten un ultrasonido torácico positivo y se encuentren hemodinámicamente estables se les debe realizar una ventana pericárdica con posterior lavado. Se ha demostrado que el 25% de las ventanas pericárdicas positivas no se benefician ni requieren de posteriores abordajes quirúrgicos invasivos. Antes de este concepto, todos los pacientes con ventana pericárdica positiva terminaban en una exploración abierta del tórax y del pericárdico.Los pacientes hemodinámicamente inestables requieren de una cirugía de control de daños para un adecuado y oportuno control del sangrado. Con este propósito, se propone un algoritmo de manejo quirúrgico que incluye todos estos aspectos esenciales en el abordaje de este grupo de pacientes.
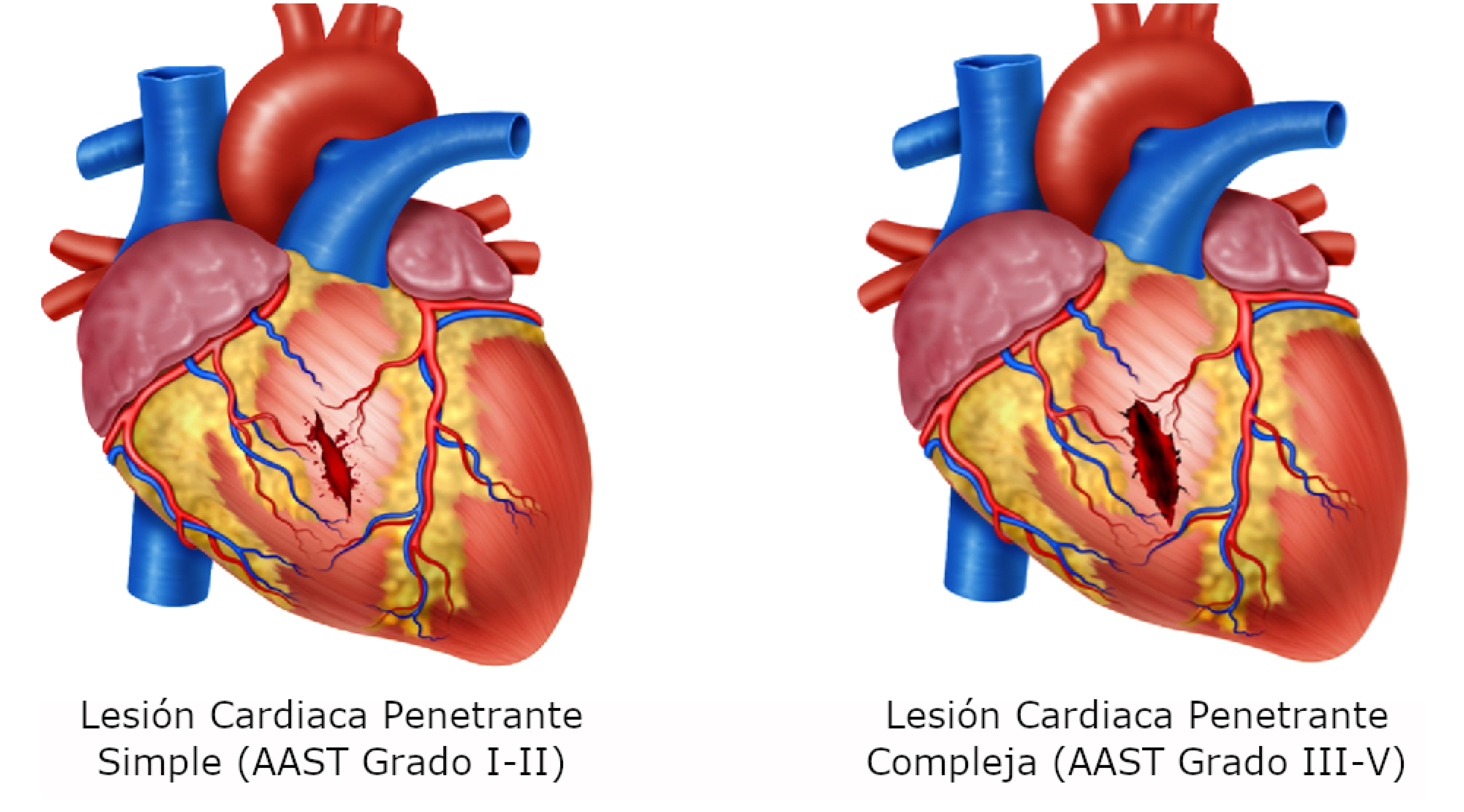
Keywords: Damage Control Surgery; Penetrating cardiac trauma; Thoracic Ultrasound; advanced trauma life support care; cardiac tamponade; chest tubes; death, sudden; hemothora; negative-pressure wound therapy; pericardial window techniques; pericardiectomy; pneumothorax; sternotomy; thoracotomy.
Copyright © 2021 Colombia Medica.
Conflict of interest statement
Conflicts of interest: The authors declare that they have no conflict of interest.
Figures
References
-
- Mugala DD, Makupe A, Ziddulla , Sakala D, Simon M, Chibale B. Occurrence of penetrating chest and hearts injury following assaults a presentation of two cases. MOJ Clin Med Case Reports. 2018;8:88–94. doi: 10.15406/mojcr.2018.08.00247. - DOI
-
- Nicol AJ. Cardiac Hemorrhage: Treatment of the Bleeding Heart. In: Ball CG, Dixon E, editors. Treatment of Ongoing Hemorrhage: The Art and Craft of Stopping Severe Bleeding. Springer; 2018. pp. 67–80.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
