

Intravenous iron therapy and the cardiovascular system: risks and benefits
- PMID: 34188903
- PMCID: PMC8223589
- DOI: 10.1093/ckj/sfaa212
Intravenous iron therapy and the cardiovascular system: risks and benefits
Abstract
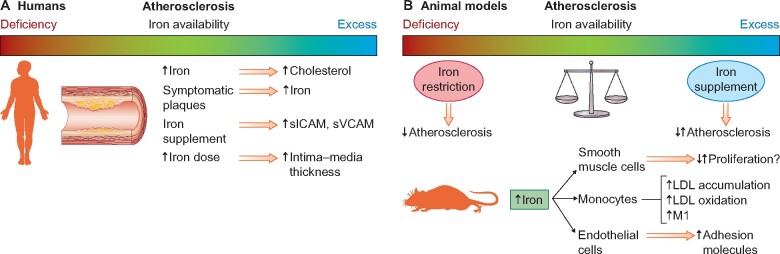
Anaemia is a common complication of chronic kidney disease (CKD). In this setting, iron deficiency is frequent because of the combination of increased iron needs to sustain erythropoiesis with increased iron losses. Over the years, evidence has accumulated on the involvement of iron in influencing pulmonary vascular resistance, endothelial function, atherosclerosis progression and infection risk. For decades, iron therapy has been the mainstay of therapy for renal anaemia together with erythropoiesis-stimulating agents (ESAs). Despite its long-standing use, grey areas still surround the use of iron therapy in CKD. In particular, the right balance between either iron repletion with adequate therapy and the avoidance of iron overload and its possible negative effects is still a matter of debate. This is particularly true in patients having functional iron deficiency. The recent Proactive IV Iron Therapy in Haemodialysis Patients trial supports the use of intravenous (IV) iron therapy until a ferritin upper limit of 700 ng/mL is reached in haemodialysis patients on ESA therapy, with short dialysis vintage and minimal signs of inflammation. IV iron therapy has also been proven to be effective in the setting of heart failure (HF), where it improves exercise capacity and quality of life and possibly reduces the risk of HF hospitalizations and cardiovascular deaths. In this review we discuss the risks of functional iron deficiency and the possible benefits and risks of iron therapy for the cardiovascular system in the light of old and new evidence.
Keywords: anaemia; cardiovascular disease; chronic kidney disease; ferritin; haemodialysis; heart failure; iron.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures

References
-
- Kidney Disease: Improving Global Outcomes Anemia Work Group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 2012; 2: 279–335
-
- Locatelli F, Bárány P, Covic A et al. Kidney Disease: Improving Global Outcomes guidelines on anaemia management in chronic kidney disease: a European Renal Best Practice position statement. Nephrol Dial Transplant 2013; 28: 1346–1359 - PubMed
-
- Macdougall IC, White C, Anker SD et al. Intravenous iron in patients undergoing maintenance hemodialysis. N Engl J Med 2019; 380: 447–458 - PubMed
-
- Ganz T. Systemic iron homeostasis. Physiol Rev 2013; 93: 1721–1741 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
