

Case Reports
doi: 10.1002/ccr3.4262.
eCollection 2021 Jun.
Pleural empyema associated with alveolar-pleural fistulas in severe acute respiratory syndrome coronavirus 2
Affiliations
- PMID: 34188928
- PMCID: PMC8218321
- DOI: 10.1002/ccr3.4262
Item in Clipboard
Case Reports
Pleural empyema associated with alveolar-pleural fistulas in severe acute respiratory syndrome coronavirus 2
Clin Case Rep.
.
Abstract
Surgery in COVID-19 disease complicated by APF represents the last life-saving treatment option. The choice of the therapeutic period to indicate this approach is fundamental. In fact, the clinical stability of patient is necessary in order to allow single-lung ventilation and to minimize postoperative sequelae.
Keywords: COVID‐19 infection; alveolar‐pleural fistula; empyema; prolonged air leaks; surgical treatment.
© 2021 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
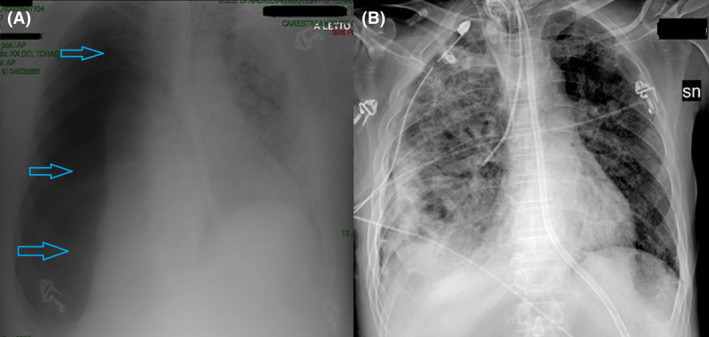
A, Large right pneumothorax (light blue arrows), associated with massive collapse of the homolateral lung; B, Parenchymal re‐expansion after pleural drainage insertion

Persistent right pneumothorax (light blue arrows) associated with pleural space infection (red arrows)

Apical and basal right pneumothorax (yellow arrows) with collapse and atelectasis of the pulmonary parenchyma. Pleural drainage is clearly visible (blue ring). Some air cavitations (orange arrows) are recognized in the lower lobe. These show serpiginous morphology as bronchiectasis and lobulated morphology as pneumatocele. Furthermore, there is a pleural effusion (red arrows) with hyperdense and irregular aspects as corpuscular component

Bilaterally, diffused ground‐glass (green arrows) and interstitial lung disease with an increase in the thickness of the septa are recognized, associated with a basal parenchymal consolidation of the left lower lobe. Moreover, paraseptal emphysema changes are also recognized

A, Arteriole occluded with micro‐channeling aspect (white arrow), intimal hyperplasia, and siderophages (blue arrows). Chronic peribronchiolar inflammation (green arrows) coexists; B, Thrombosed arterioles (red arrow) associated with an intense inflammatory reaction (green arrows) and micro‐channeling aspects (white arrows); C, Subpleural pulmonary parenchyma with intense inflammation (green arrow). The bronchiole shows fistula (black arrows) and extensive squamous metaplasia (orange arrows). On the side, a thrombosed artery (red arrow) due to intimal hyperplasia with vascular micro‐recanalization (white arrow) is observed; D, Alveolar‐pleural fistula (black arrows), with squamous metaplasia (orange arrows) of bronchial epithelium

A, The bronchiole with squamous metaplasia (orange arrows); B, Thickened lung interstitium, with inflammatory elements and macrophages (white rings) that have phagocytized hemosiderin (siderophages, outcome of hemorrhage). Alveoli collapsed (light blue arrows) with endoalveolar foamy macrophages are also noted; C, Thrombosed arteriole (red arrows) in which a minimal vascular lumen (white arrows) can be appreciated; D, Pulmonary parenchyma with extensive necrosis (gray arrows), surrounding inflammatory lymphocytes and infiltration of granulocyte neutrophils (blue arrow). Residual vascular structures (yellow arrow) with wall necrosis are also observed
References
Publication types
LinkOut - more resources
Full Text Sources
