

Narrative review of congenital lung lesions
- PMID: 34189102
- PMCID: PMC8192987
- DOI: 10.21037/tp-20-133
Narrative review of congenital lung lesions
Abstract
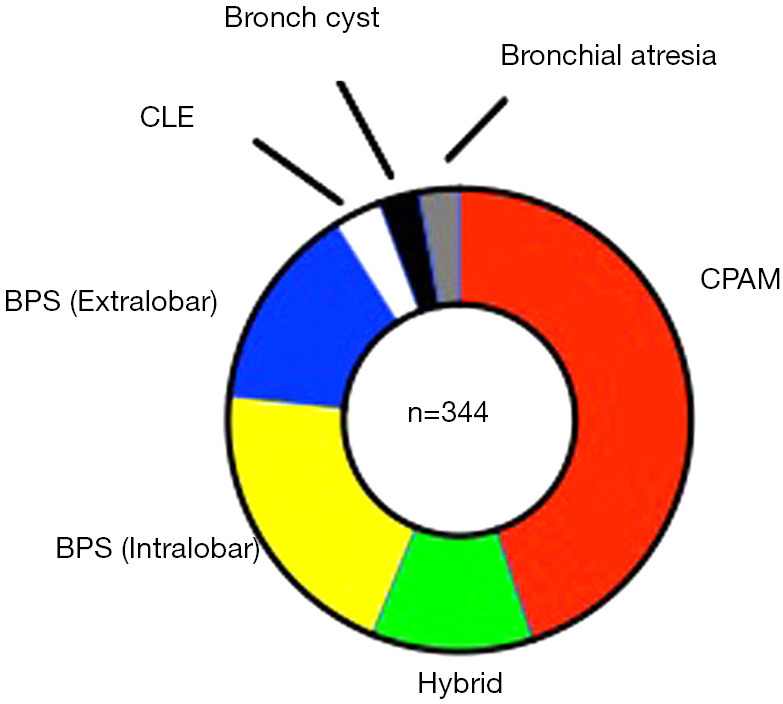
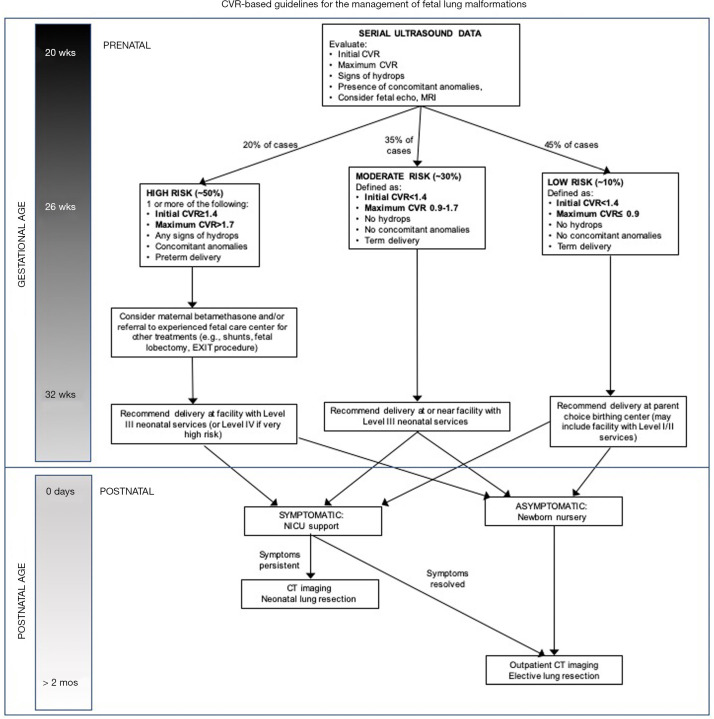
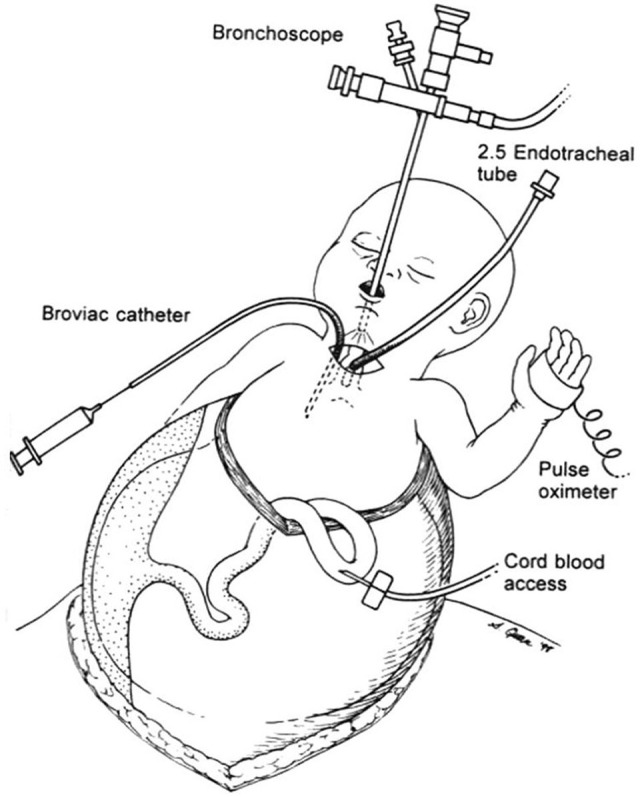
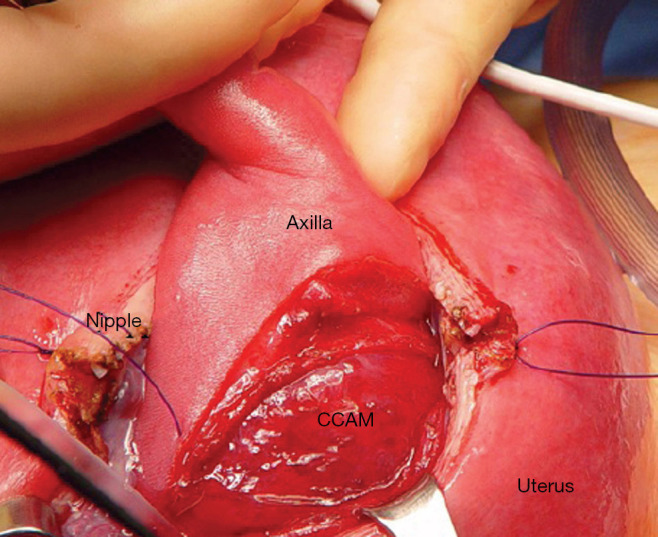
This article reviews the contemporary diagnosis and management of antenatally diagnosed congenital lung lesions. These anomalies, which include congenital pulmonary airway malformation (CPAM) (formerly congenital cystic adenomatoid malformation), bronchopulmonary sequestration (BPS), bronchogenic cyst, and congenital lobar emphysema (CLE), are relatively rare but are increasingly encountered by clinicians because of the improved resolution and enhanced sensitivity of fetal ultrasound. Serial assessment of these lesions throughout pregnancy remains the norm rather than the exception. Perinatal management strategies may differ based on initial size and growth patterns of these masses until delivery. Fetal magnetic resonance imaging and other diagnostic testing can sometimes be helpful in providing additional prognostic information. Over the last decade, maternal steroids have become standard of care in the management of larger lesions at risk for nonimmune hydrops. As a result, fetal surgical procedures, including open resection, thoracoamniotic shunting, and ex utero intrapartum treatment (EXIT), are less uncommonly performed. Decisions regarding whether delivery of these fetuses should occur in a tertiary care center with pediatric surgery coverage versus delivery at a local community hospital are now highly relevant in most prenatal counseling discussions with families. Large lung malformations may require urgent surgical removal in the early postnatal period because of respiratory distress. Other complications, such as recurrent pneumonia, pneumothorax, and cancer, are indications for postnatal lung resection on an elective basis. Many children are good candidates for minimally invasive (thoracoscopic) surgical approaches as an alternative to resection by thoracotomy. In the vast majority of cases, the overall prognosis remains excellent.
Keywords: Congenital lung lesion; bronchopulmonary sequestrations (BPS); congenital pulmonary airway malformations (CPAM); fetal surgery.
2021 Translational Pediatrics. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The author has completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tp-20-133). The series “Fetal Surgery” was commissioned by the editorial office without any funding or sponsorship. The author has no other conflicts of interest to declare.
Figures





Similar articles
-
Management of perinatal lung malformations.Minerva Ginecol. 2015 Feb;67(1):81-94. Epub 2014 Oct 13. Minerva Ginecol. 2015. PMID: 25310108 Review.
-
Fetal lung lesions: management and outcome.Am J Obstet Gynecol. 1998 Oct;179(4):884-9. doi: 10.1016/s0002-9378(98)70183-8. Am J Obstet Gynecol. 1998. PMID: 9790364
-
Congenital lung malformations--antenatal and postnatal evaluation and management.Eur J Cardiothorac Surg. 2005 Jan;27(1):45-52. doi: 10.1016/j.ejcts.2004.10.015. Eur J Cardiothorac Surg. 2005. PMID: 15621470
-
Two's Company: Multiple Thoracic Lesions on Prenatal US and MRI.Fetal Diagn Ther. 2020;47(8):642-652. doi: 10.1159/000507783. Epub 2020 Jun 29. Fetal Diagn Ther. 2020. PMID: 32599594
-
Congenital cystic lung disease: contemporary antenatal and postnatal management.Pediatr Surg Int. 2008 Jun;24(6):643-57. doi: 10.1007/s00383-008-2139-3. Epub 2008 Apr 5. Pediatr Surg Int. 2008. PMID: 18392629 Review.
Cited by
-
Invasive Mucinous Adenocarcinoma in a Newborn With Antenatally Diagnosed Congenital Pulmonary Airway Malformation: A Case Report.Cureus. 2024 Aug 3;16(8):e66063. doi: 10.7759/cureus.66063. eCollection 2024 Aug. Cureus. 2024. PMID: 39229431 Free PMC article.
-
Effects of pulmonary fissure completeness on major outcomes in children after video-assisted thoracoscopic congenital lung malformation lobectomy.BMC Pediatr. 2022 Aug 1;22(1):462. doi: 10.1186/s12887-022-03527-4. BMC Pediatr. 2022. PMID: 35915489 Free PMC article.
-
Congenital pulmonary airway malformation type 2 associated with intralobar pulmonary sequestration in an adult patient: a case report.Future Sci OA. 2025 Dec;11(1):2527473. doi: 10.1080/20565623.2025.2527473. Epub 2025 Jul 2. Future Sci OA. 2025. PMID: 40600506 Free PMC article.
-
Antenatal diagnosis of bronchopulmonary sequestration: A case report and review of the literature.Radiol Case Rep. 2023 Nov 24;19(2):604-613. doi: 10.1016/j.radcr.2023.10.061. eCollection 2024 Feb. Radiol Case Rep. 2023. PMID: 38111561 Free PMC article.
-
A rare case of symptomatic congenital lobar emphysema in an adolescent female who underwent expectant management of a congenital pulmonary malformation: a case report.AME Case Rep. 2024 Sep 4;8:98. doi: 10.21037/acr-24-28. eCollection 2024. AME Case Rep. 2024. PMID: 39380861 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials