

Twin to twin transfusion syndrome
- PMID: 34189110
- PMCID: PMC8193008
- DOI: 10.21037/tp-20-264
Twin to twin transfusion syndrome
Abstract
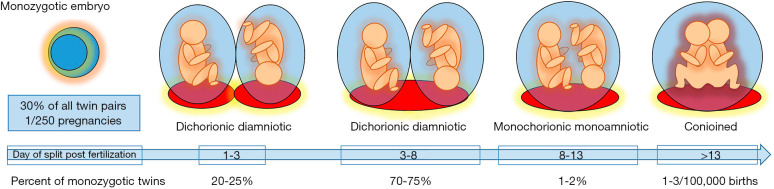
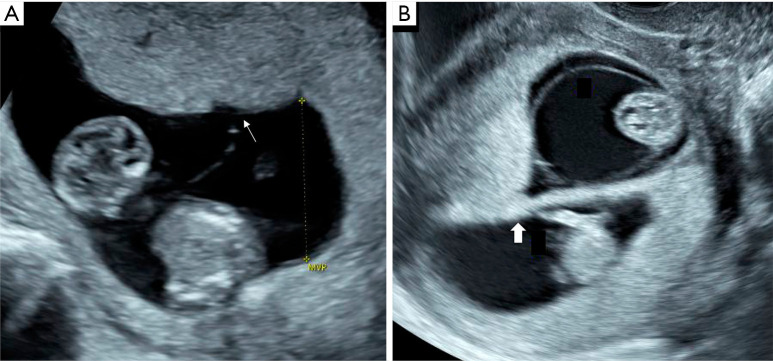
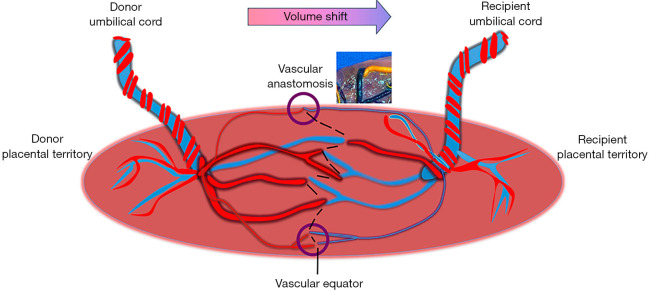
Twin to twin transfusion syndrome (TTTS) is a common complication that typically presents in the second trimester of pregnancy in 10-15% of monochorionic twins due to net transfer of volume and hormonal substances from one twin to the other across vascular anastomoses on the placenta. Without recognition and treatment, TTTS is the greatest contributor to fetal loss prior to viability in 90-100% of advanced cases. Ultrasound diagnosis of monochorionicity is most reliable in the first trimester and sets the monitoring strategy for this type of twins. The diagnosis of TTTS is made by ultrasound with the findings of polyhydramnios due to volume overload and polyuria in one twin and oligohydramnios due to oliguria of the co-twin. Assessment of bladder filling as well as arterial and venous Doppler patterns are required for staging disease severity. Assessment of fetal cardiac function also provides additional insight into the fetal cardiovascular impacts of the disease as well as help identify fetuses that may require postnatal follow up. Fetoscopic laser ablation of the communicating vascular anastomoses between the twins is the standard treatment for TTTS. It aims to cure the condition by interrupting the link between their circulations and making them independent of one another. Contemporary outcome data after laser surgery suggests survival for both fetuses can be anticipated in up to 65% of cases and survival of a single fetus in up to 88% of cases. However, preterm birth remains a significant contributor to postnatal morbidity and mortality. Long term outcomes of TTTS survivors indicate that up to 11% of children may show signs of neurologic impairment. Strategies to minimize preterm birth after treatment and standardized reporting by laser centers are important considerations to improve overall outcomes and understand the long-term impacts of TTTS.
Keywords: Fetoscopy; placental diseases, pregnancy, twin; twin to twin transfusion syndrome (TTTS).
2021 Translational Pediatrics. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The author has completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tp-20-264). The series “Fetal Surgery” was commissioned by the editorial office without any funding or sponsorship. The author has no other conflicts of interest to declare.
Figures
References
-
- Carroll SGM, Soothill PW, Abdel-Fattah SA, et al. Prediction of chorionicity in twin pregnancies at 10-14 weeks of gestation. BJOG 2002;109:182-6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources