

Randomized phase 2 study of perampanel for sporadic amyotrophic lateral sclerosis
- PMID: 34191081
- PMCID: PMC8782807
- DOI: 10.1007/s00415-021-10670-y
Randomized phase 2 study of perampanel for sporadic amyotrophic lateral sclerosis
Abstract
Objective: To evaluate the efficacy and safety of perampanel in patients with sporadic amyotrophic lateral sclerosis (SALS).
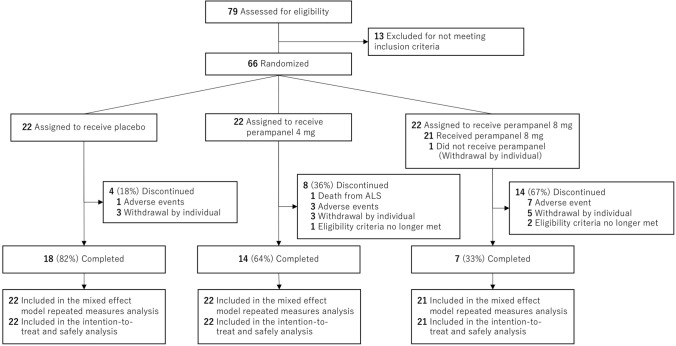
Methods: This randomized, double-blind, placebo-controlled, multicenter, phase 2 clinical study was conducted at 12 sites. Patients with probable or definite ALS as defined by revised El Escorial criteria were enrolled. Sixty-six patients were randomly assigned (1:1:1) to receive placebo, 4 mg perampanel, or 8 mg perampanel daily for 48 weeks. Adverse events (AEs) were recorded throughout the trial period. The primary efficacy outcome was the change in Amyotrophic Lateral Sclerosis Rating Scale-Revised (ALSFRS-R) score after 48 weeks of treatment.
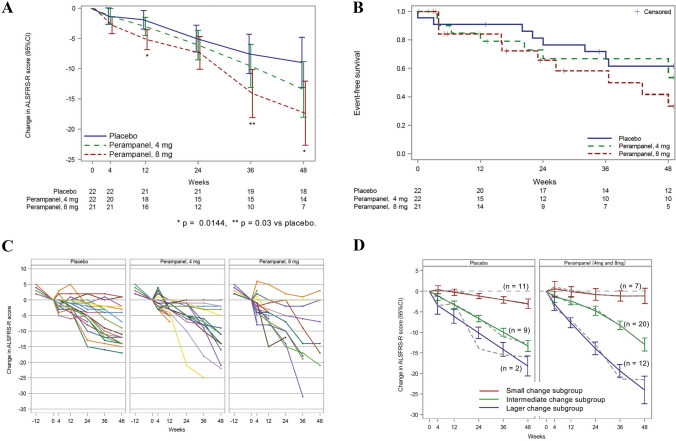
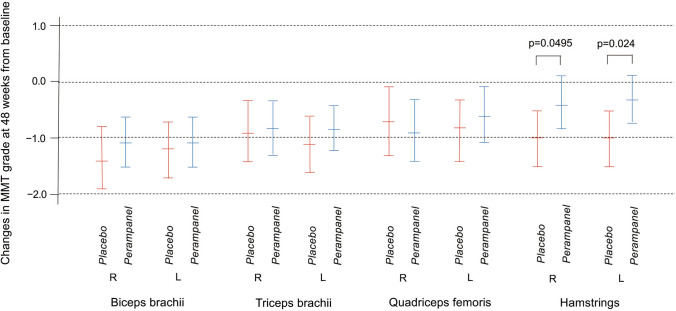
Results: One patient withdrew before starting the treatment. Of 65 patients included, 18 of 22 patients randomized to placebo (82%), 14 of 22 patients randomized to 4 mg perampanel (64%), and 7 of 21 patients randomized to 8 mg perampanel (33%) completed the trial. There was a significant difference in the change of ALSFRS-R scores [- 8.4 (95% CI - 13.9 to - 2.9); p = 0.015] between the placebo and the perampanel 8 mg group, primarily due to worsening of the bulbar subscore in the perampanel 8 mg group. Serious AEs were more frequent in the perampanel 8 mg group than in the placebo group (p = 0.0483).
Conclusions: Perampanel was associated with a significant decline in ALSFRS-R score and was linked to worsening of the bulbar subscore in the 8 mg group.
Keywords: AMPA receptor; Efficacy; Perampanel; Safety; Sporadic amyotrophic lateral sclerosis.
© 2021. The Author(s).
Conflict of interest statement
K.O. reports receiving honoraria from Takeda Pharmaceutical Co., Ltd, Ono Pharmaceutical Co., Ltd, Eisai Co., Ltd, Chugai Pharmaceutical Co, Ltd., and Daiichi Sankyo Co., Ltd., outside the submitted work. M.K. reports receiving grants from AMED, Japan, during the conduct of the study; receiving grants from Mitsubishi Tanabe Pharma, grants from Sanofi, and consulting fees from Eisai, outside the submitted work. N.A. reports receiving grants from the Center for Clinical Trials, Japan Medical Association, during the conduct of the study. H.I. reports receiving speaker fees from Eisai, outside the submitted work. M.A. reports receiving research grants for Research on Nervous and Mental Disorders, Research on Rare and Intractable Diseases, Research on Psychiatric and Neurological Diseases and Mental Health from the Japanese Ministry of Health Labor and Welfare; Grants-in-Aid for Scientific Research, an Intramural Research Grant for Neurological Psychiatric Disorders from National Center of Neurology and Psychiatry (NCNP); Grants-in-Aid for Scientific Research from the Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT); and a grants of Practical Research Project for Rare/Intractable Diseases from the Japan Agency for Medical Research and Development (AMED); and funding for travel and speaker honoraria from Eisai Inc., Mitsubishi Tanabe Pharma Corporation, Astellas Pharma Inc., Takeda Pharmaceutical Company Ltd, Sanofi K.K. Novartis Pharma K.K and Dainippon Sumitomo Pharma Co. Ltd. H.M. reports receiving grants from the Japan Agency for Medical Research and Development and grants from the Japanese Ministry of Health, Labor and Welfare, outside the submitted work. The other authors have nothing to report.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
