

Optimizing outcomes of ACL surgery-Is autograft reconstruction the only reasonable option?
- PMID: 34191344
- PMCID: PMC8387392
- DOI: 10.1002/jor.25128
Optimizing outcomes of ACL surgery-Is autograft reconstruction the only reasonable option?
Abstract
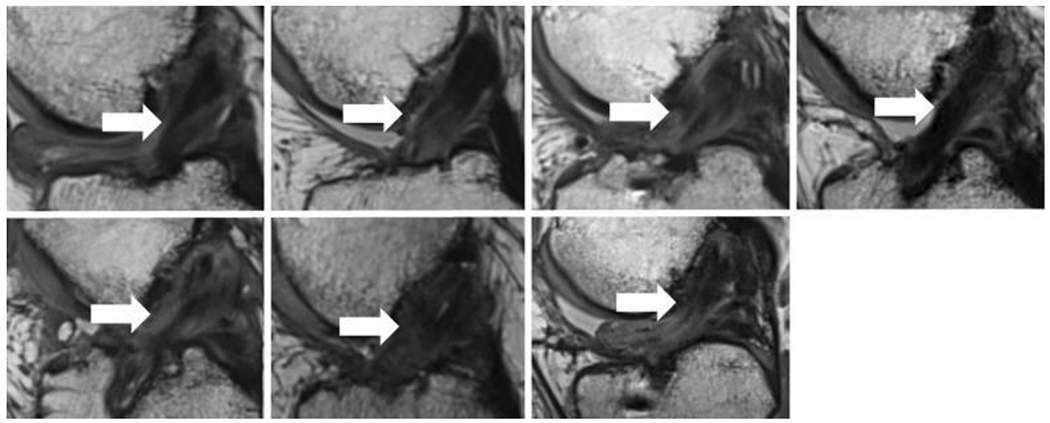
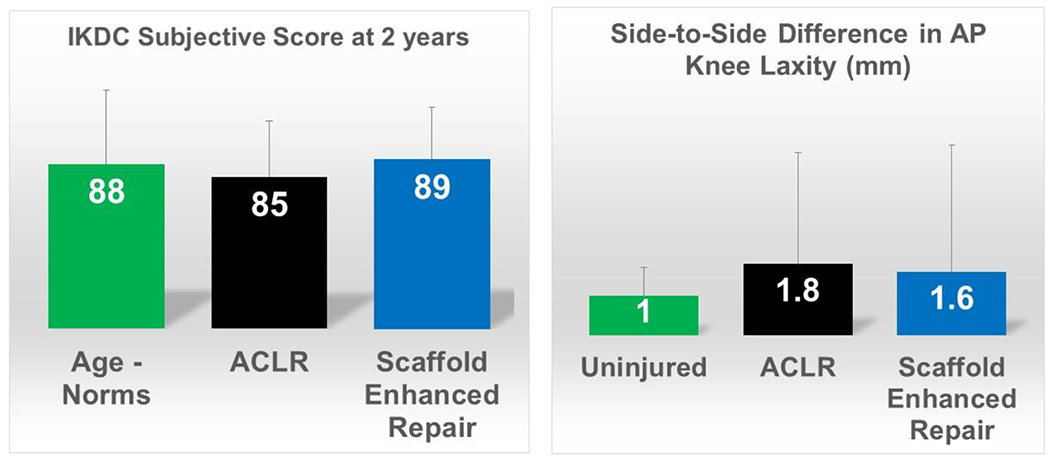
Anterior cruciate ligament (ACL) injuries occur at a high frequency in the United States with approximately 400,000 ACL reconstructions being performed each year. While ACL reconstruction is our current gold standard of treatment, it does not restore joint motion, or prevent the premature development of posttraumatic osteoarthritis (PTOA) in many patients. Thus, new treatments for an ACL injury, which are less invasive and minimize patient morbidity, including cartilage damage, are highly desirable. We have used a tissue-engineered approach to stimulate ligament healing, to improve upon current treatment options. In this review, we describe and discuss our work moving a tissue engineering strategy from the concept to bench, preclinical, clinical trials and ultimately FDA 510(k) de Novo approval, providing clinicians and patients with a viable alternative to ACL reconstruction.
Keywords: ACL reconstruction; ACL repair; anterior cruciate ligament; bridge-enhanced ACL repair; clinical trial; platelet; posttraumatic osteoarthritis; scaffold-enhanced ACL repair; tissue engineering.
© 2021 Orthopaedic Research Society. Published by Wiley Periodicals LLC.
Figures
References
-
- Junkin DM, Johnson DL, Fu FH, et al.2009. Knee Ligament Injuries. In: Kibler WB editor. Orthopaedic Knowledge Update:Sports Medicine. Rosemont, IL: American Academy of Orthopaedic Surgeons; p. 136.
-
- Beynnon BD, Uh BS, Johnson RJ, et al.2005. Rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind comparison of programs administered over 2 different time intervals. Am J Sports Med 33:347–359. - PubMed
-
- Fleming BC, Brattbakk B, Peura GD, et al.2002. Measurement of anterior-posterior knee laxity: a comparison of three techniques. J Orthop Res 20:421–426. - PubMed
-
- Tashman S, Kolowich P, Collon D, et al.2007. Dynamic function of the ACL-reconstructed knee during running. Clin Orthop Relat Res 454:66–73. - PubMed
-
- Lohmander LS, Ostenberg A, Englund M, et al.2004. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum 50:3145–3152. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
