

Plasma ACE2 species are differentially altered in COVID-19 patients
- PMID: 34191346
- PMCID: PMC8441911
- DOI: 10.1096/fj.202100051R
Plasma ACE2 species are differentially altered in COVID-19 patients
Erratum in
-
Erratum.FASEB J. 2021 Sep;35(9):e21857. doi: 10.1096/fsb2.21857. FASEB J. 2021. PMID: 34403542 Free PMC article. No abstract available.
Abstract
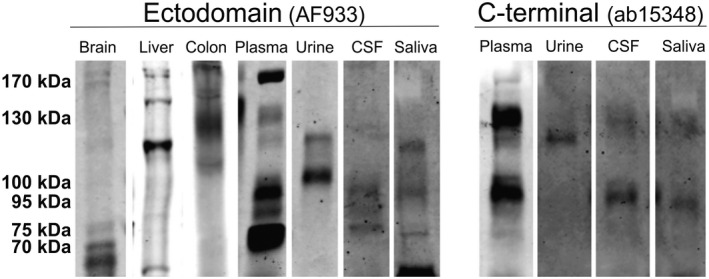
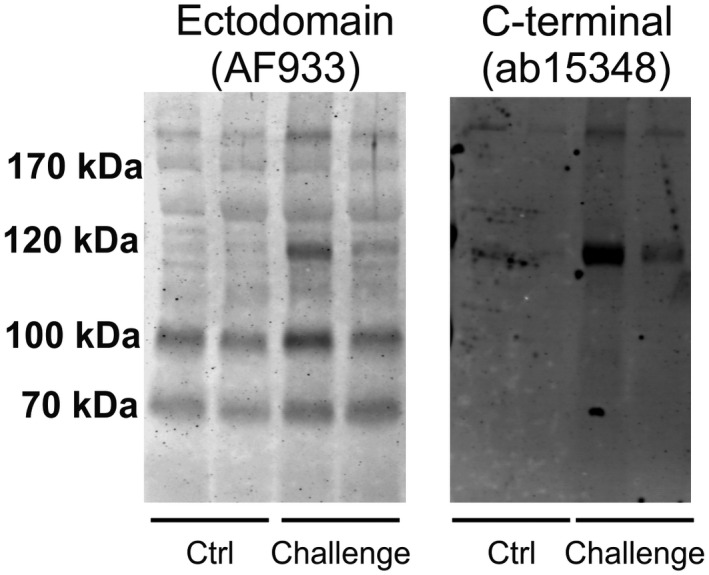
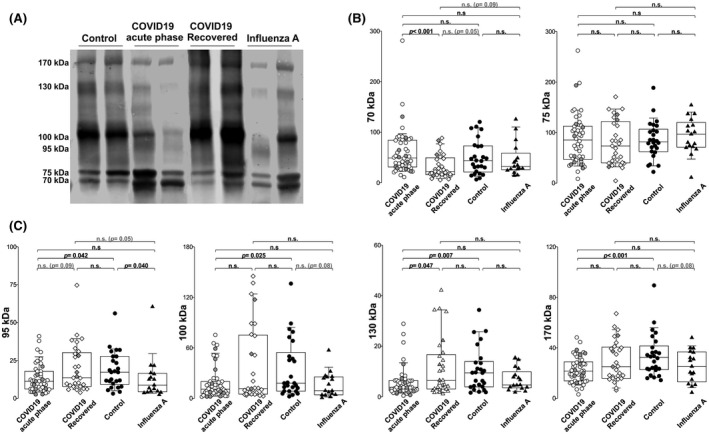
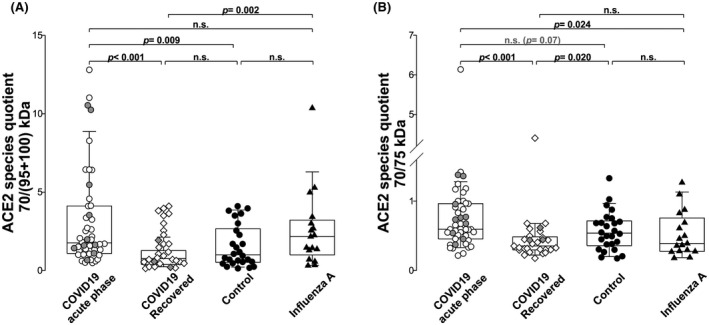
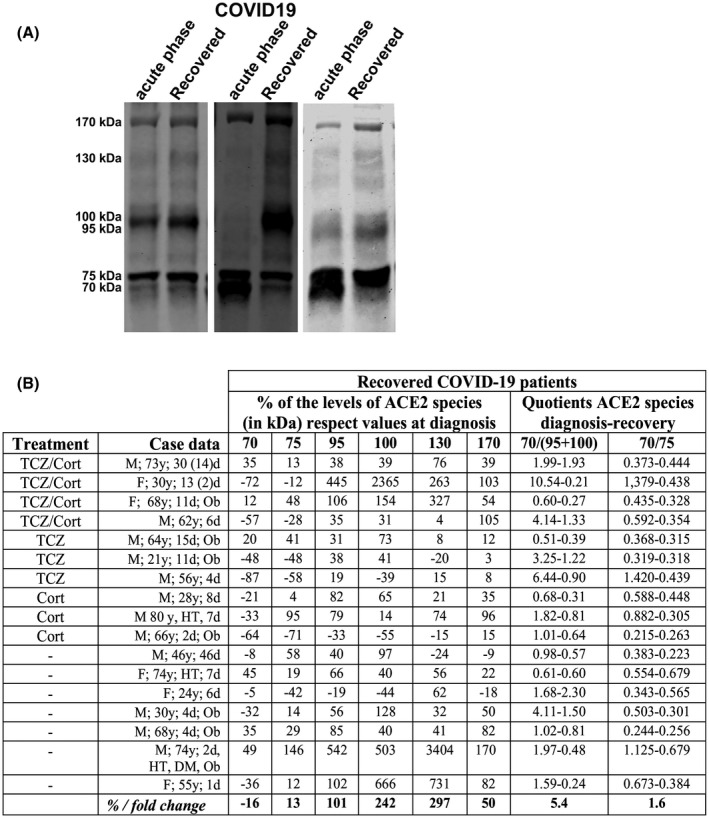
Studies are needed to identify useful biomarkers to assess the severity and prognosis of COVID-19 disease, caused by severe acute respiratory syndrome coronavirus (SARS-CoV-2) virus. Here, we examine the levels of various plasma species of the SARS-CoV-2 host receptor, the angiotensin-converting enzyme 2 (ACE2), in patients at different phases of the infection. Human plasma ACE2 species were characterized by immunoprecipitation and western blotting employing antibodies against the ectodomain and the C-terminal domain, using a recombinant human ACE2 protein as control. In addition, changes in the cleaved and full-length ACE2 species were also examined in serum samples derived from humanized K18-hACE2 mice challenged with a lethal dose of SARS-CoV-2. ACE2 immunoreactivity was present in human plasma as several molecular mass species that probably comprise truncated (70 and 75 kDa) and full-length forms (95, 100, 130, and 170 kDa). COVID-19 patients in the acute phase of infection (n = 46) had significantly decreased levels of ACE2 full-length species, while a truncated 70-kDa form was marginally higher compared with non-disease controls (n = 26). Levels of ACE2 full-length species were in the normal range in patients after a recovery period with an interval of 58-70 days (n = 29), while the 70-kDa species decreased. Levels of the truncated ACE2 species served to discriminate between individuals infected by SARS-CoV-2 and those infected with influenza A virus (n = 17). In conclusion, specific plasma ACE2 species are altered in patients with COVID-19 and these changes normalize during the recovery phase. Alterations in ACE2 species following SARS-CoV-2 infection warrant further investigation regarding their potential usefulness as biomarkers for the disease process and to asses efficacy during vaccination.
Keywords: ACE2; COVID-19; SARS-CoV-2; biomarker; plasma.
© 2021 The Authors. The FASEB Journal published by Wiley Periodicals LLC on behalf of Federation of American Societies for Experimental Biology.
Conflict of interest statement
All the authors declare that they have no competing interest.
Figures

References
-
- Tipnis SR, Hooper NM, Hyde R, et al. A human homolog of angiotensin‐converting enzyme. Cloning and functional expression as a captopril‐insensitive carboxypeptidase. J Biol Chem. 2000;275(43):33238‐33243. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
