

Case Studies in Neuroscience: Neuropathology and diaphragm dysfunction in ventilatory failure from late-onset Pompe disease
- PMID: 34191636
- PMCID: PMC8409957
- DOI: 10.1152/jn.00190.2021
Case Studies in Neuroscience: Neuropathology and diaphragm dysfunction in ventilatory failure from late-onset Pompe disease
Abstract
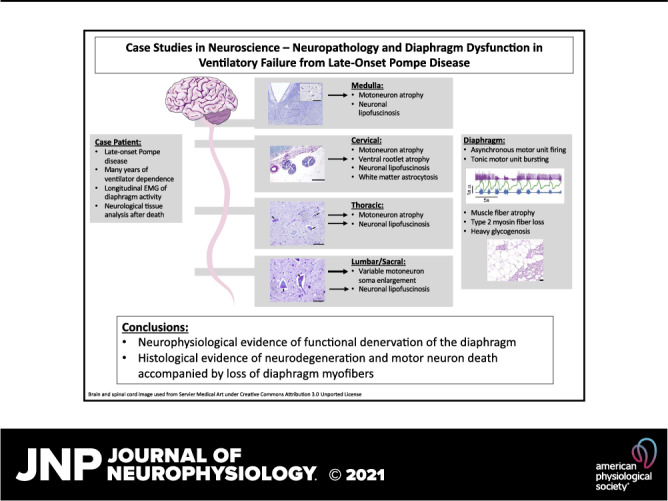
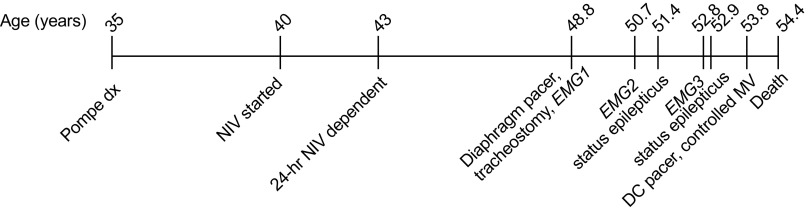
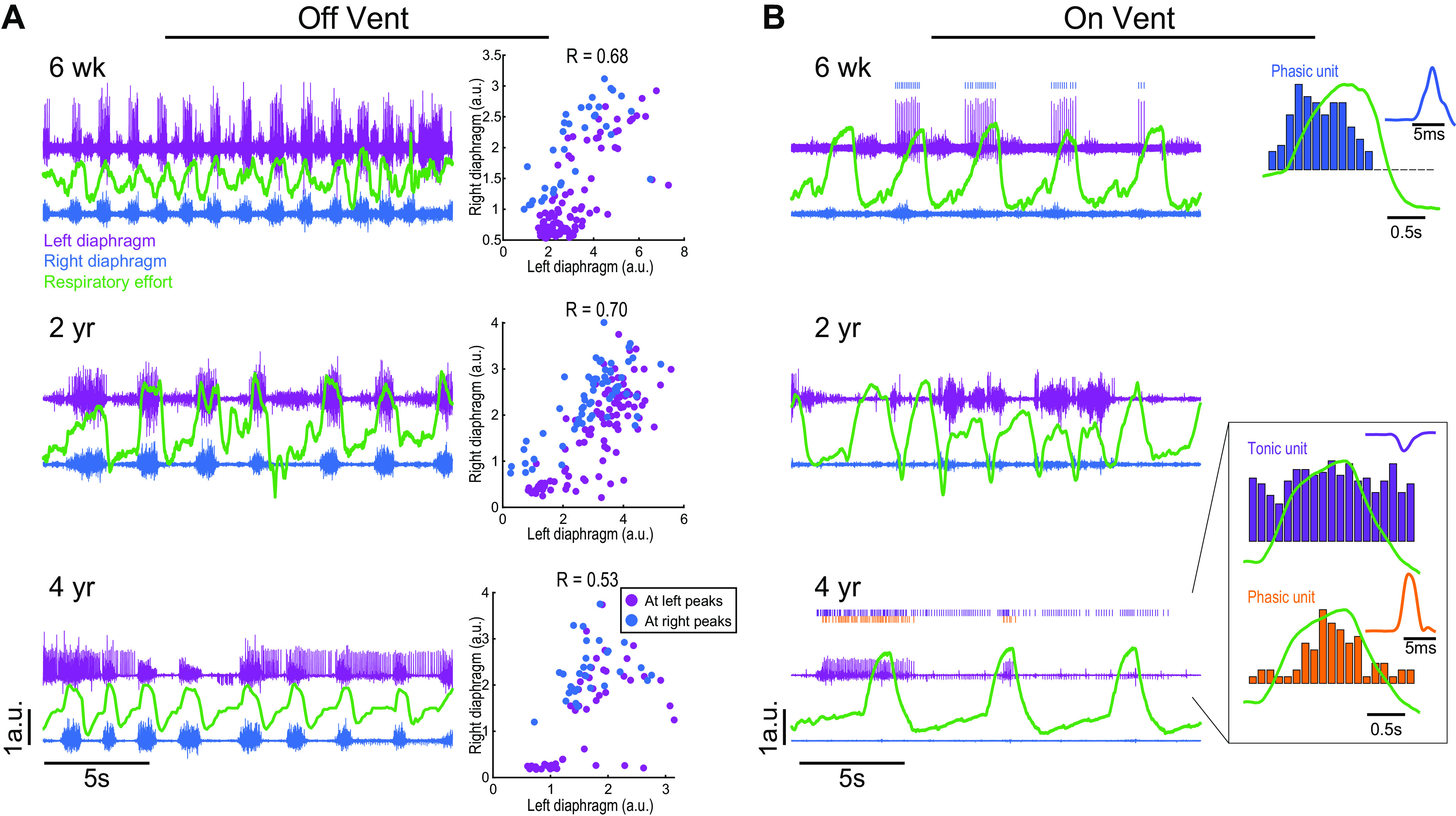
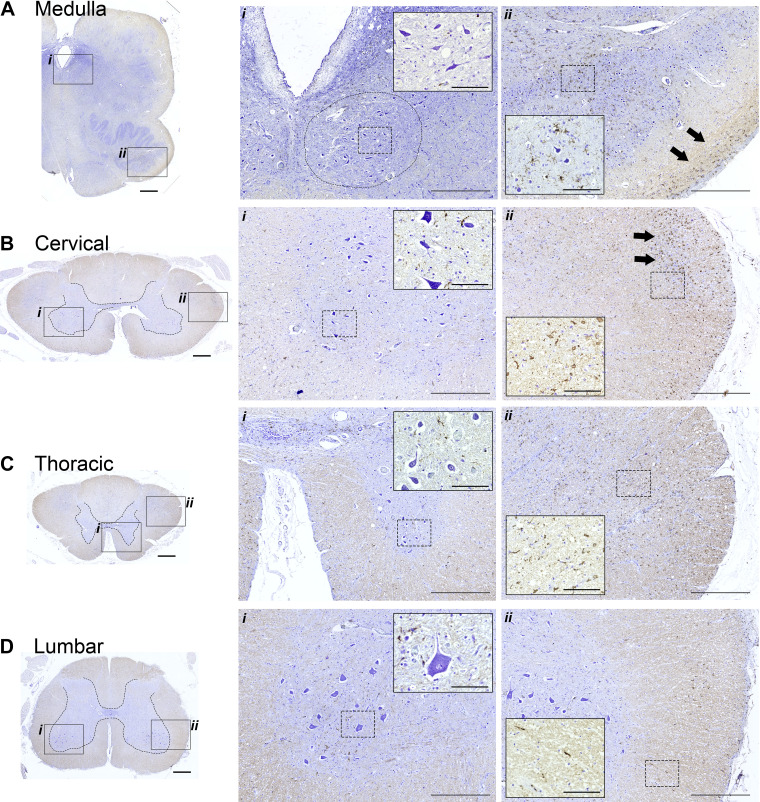
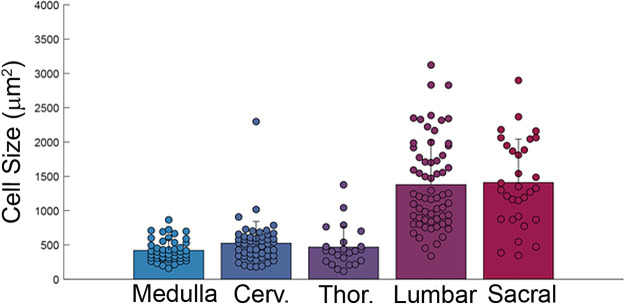
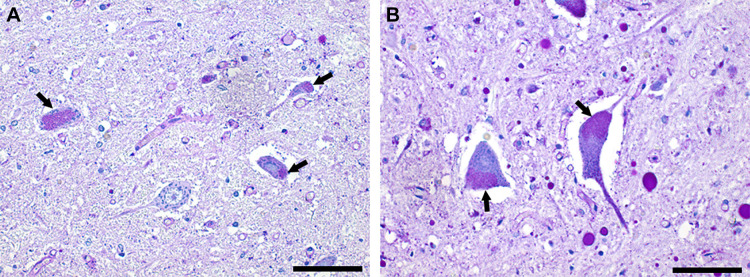
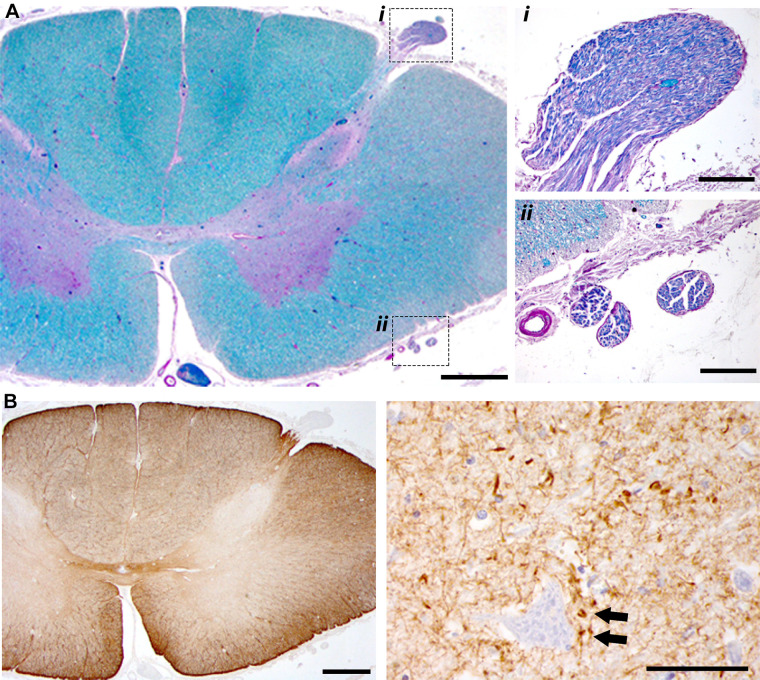
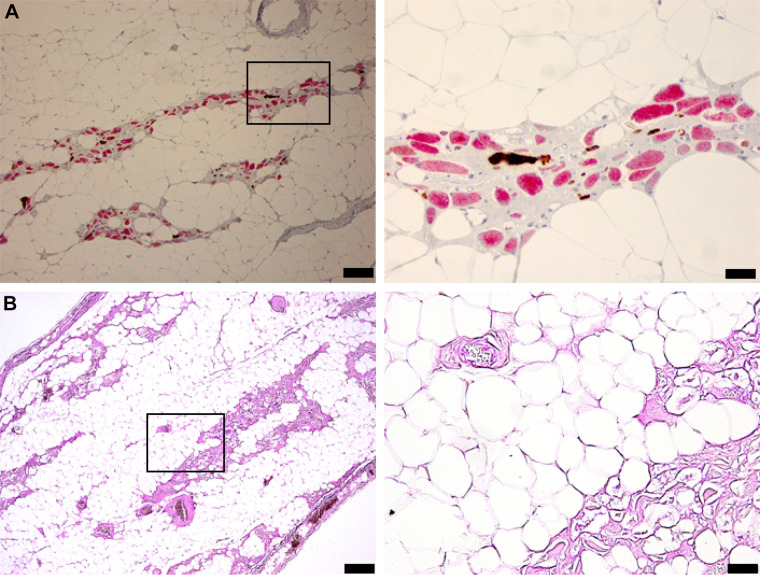
Pompe disease (PD) is a neuromuscular disorder caused by a mutation in the acid alpha-glucosidase (GAA) gene. Patients with late-onset PD retain some GAA activity and present symptoms later in life, with fatality mainly associated with respiratory failure. This case study presents diaphragm electrophysiology and a histological analysis of the brainstem, spinal cord, and diaphragm, from a male PD patient diagnosed with late-onset PD at age 35. The patient was wheelchair dependent by age 38, required nocturnal ventilation at age 40, 24-h noninvasive ventilation by age 43, and passed away from respiratory failure at age 54. Diaphragm electromyography recorded using indwelling "pacing" wires showed asynchronous bursting between the left and right diaphragm during brief periods of independent breathing. The synchrony declined over a 4-yr period preceding respiratory failure. Histological assessment indicated motoneuron atrophy in the medulla and rostral spinal cord. Hypoglossal (soma size: 421 ± 159 µm2) and cervical motoneurons (soma size: 487 ± 189 µm2) had an atrophied, elongated appearance. In contrast, lumbar (soma size: 1,363 ± 677 µm2) and sacral motoneurons (soma size: 1,411 ± 633 µm2) had the ballooned morphology typical of early-onset PD. Diaphragm histology indicated loss of myofibers. These results are consistent with neuromuscular degeneration and the concept that effective PD therapy will need to target the central nervous system, in addition to skeletal and cardiac muscle.NEW & NOTEWORTHY This case study offered a unique opportunity to investigate longitudinal changes in phrenic neurophysiology in an individual with severe, ventilator-dependent, late-onset Pompe disease. Additional diaphragm and neural tissue histology upon autopsy confirmed significant neuromuscular degeneration, and it provided novel insights regarding rostral to caudal variability in the neuropathology. These findings suggest that a successful treatment approach for ventilator-dependent Pompe disease should target the central nervous system, in addition to skeletal muscle.
Keywords: Pompe disease; diaphragm; neuropathology; respiratory; spinal cord.
Conflict of interest statement
B.J.B. is a member of the Pfizer Rare Disease Therapeutic Advisory Board and Sanofi Pompe Registry Board as well as co-founder of AavantiBio; however, the manuscript does not evaluate therapeutic interventions in Pompe disease. The author is an inventor of intellectual property related to Pompe disease, which is owned by the University of Florida. B.K.S. is an external consultant for Amicus Therapeutics.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous