

Long-term outcomes of ivermectin-albendazole versus albendazole alone against soil-transmitted helminths: Results from randomized controlled trials in Lao PDR and Pemba Island, Tanzania
- PMID: 34191812
- PMCID: PMC8277064
- DOI: 10.1371/journal.pntd.0009561
Long-term outcomes of ivermectin-albendazole versus albendazole alone against soil-transmitted helminths: Results from randomized controlled trials in Lao PDR and Pemba Island, Tanzania
Abstract
Background: Preventive chemotherapy is the cornerstone of soil-transmitted helminth (STH) control. Long-term outcomes and adequate treatment frequency of the recently recommended albendazole-ivermectin have not been studied to date.
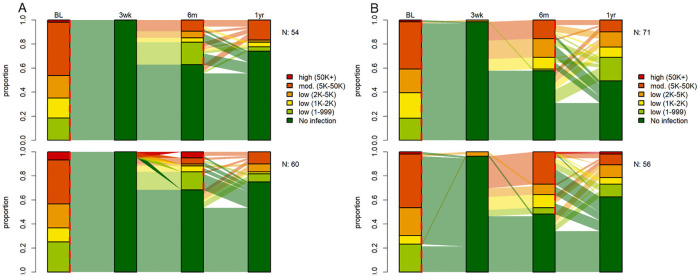
Methodology/principal findings: Double-blind randomized controlled trials were conducted in Lao PDR, Pemba Island, Tanzania and Côte d'Ivoire between 2018 and 2020 to evaluate the efficacy and safety of ivermectin-albendazole versus albendazole-placebo in Trichuris trichiura-infected individuals aged 6 to 60. In the framework of this study, in Lao PDR 466 and 413 participants and on Pemba Island, 558 and 515 participants were followed-up six and 12 months post-treatment, respectively. From each participant at least one stool sample was processed for Kato-Katz diagnosis and cure rates (CRs), egg reduction rates (ERRs) and apparent reinfection rates were calculated. If found helminth-positive at six months, participants were re-treated according to their allocated treatment. Long-term outcomes against T. trichiura based on CRs and ERRs of ivermectin-albendazole compared to albendazole were significantly higher at six months in Lao PDR (CR, 65.8 vs 13.4%, difference; 52.4; 95% CI 45.0-60.0; ERRs, 99.0 vs 79.6, difference 19.4; 95% CI 14.4-24.4) and Pemba Island (CR, 17.8 vs 1.4%, difference; 16.4; 95% CI 11.6-21.0; ERRs, 84.9 vs 21.2, difference 63.8; 95% CI 50.6-76.9) and also at 12 months in Lao PDR (CR, 74.0 vs 23.4%, difference; 50.6; 95% CI 42.6-61.0; ERRs, 99.6 vs 91.3, difference 8.3; 95% CI 5.7-10.8) and Pemba Island (CR, 19.5 vs 3.4%, difference; 16.1; 95% CI 10.7-21.5; ERRs, 92.9 vs 53.6, difference 39.3; 95% CI 31.2-47.4) respectively. Apparent reinfection rates with T. trichiura were considerably higher on Pemba Island (100.0%, 95% CI, 29.2-100.0) than in Lao PDR (10.0%, 95% CI, 0.2-44.5) at 12 months post-treatment for participants treated with albendazole alone.
Conclusions/significance: The long-term outcomes against T. trichiura of ivermectin-albendazole are superior to albendazole in terms of CRs and ERRs and in reducing infection intensities. Our results will help to guide decisions on how to best use ivermectin-albendazole in the context of large-scale PC programs tailored to the local context to sustainably control STH infections.
Trial registration: ClinicalTrials.gov registered with clinicaltrials.gov, reference: NCT03527732, date assigned: 17 May 2018.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
Efficacy and safety of co-administered ivermectin and albendazole in school-aged children and adults infected with Trichuris trichiura in Côte d'Ivoire, Laos, and Pemba Island, Tanzania: a double-blind, parallel-group, phase 3, randomised controlled trial.Lancet Infect Dis. 2022 Jan;22(1):123-135. doi: 10.1016/S1473-3099(21)00421-7. Epub 2021 Nov 29. Lancet Infect Dis. 2022. PMID: 34856181 Clinical Trial.
-
Efficacy and safety of ivermectin and albendazole co-administration in school-aged children and adults infected with Trichuris trichiura: study protocol for a multi-country randomized controlled double-blind trial.BMC Infect Dis. 2019 Mar 18;19(1):262. doi: 10.1186/s12879-019-3882-x. BMC Infect Dis. 2019. PMID: 30885157 Free PMC article.
-
Efficacy and safety of tribendimidine, tribendimidine plus ivermectin, tribendimidine plus oxantel pamoate, and albendazole plus oxantel pamoate against hookworm and concomitant soil-transmitted helminth infections in Tanzania and Côte d'Ivoire: a randomised, controlled, single-blinded, non-inferiority trial.Lancet Infect Dis. 2017 Nov;17(11):1162-1171. doi: 10.1016/S1473-3099(17)30487-5. Epub 2017 Aug 29. Lancet Infect Dis. 2017. PMID: 28864027 Clinical Trial.
-
Efficacy of Albendazole and Mebendazole Against Soil Transmitted Infections among Pre-School and School Age Children: A Systematic Review and Meta-Analysis.J Epidemiol Glob Health. 2024 Sep;14(3):884-904. doi: 10.1007/s44197-024-00231-7. Epub 2024 May 2. J Epidemiol Glob Health. 2024. PMID: 38696109 Free PMC article.
-
Efficacy of albendazole against soil-transmitted helminth infections in Ethiopia: a systematic review and meta-analysis.Sci Rep. 2024 Sep 20;14(1):21970. doi: 10.1038/s41598-024-71308-3. Sci Rep. 2024. PMID: 39304661 Free PMC article.
Cited by
-
Impact of preventive chemotherapy on transmission of soil-transmitted helminth infections in Pemba Island, United Republic of Tanzania, 1994-2021.PLoS Negl Trop Dis. 2022 Jun 27;16(6):e0010477. doi: 10.1371/journal.pntd.0010477. eCollection 2022 Jun. PLoS Negl Trop Dis. 2022. PMID: 35759453 Free PMC article.
-
Towards global control of parasitic diseases in the Covid-19 era: One Health and the future of multisectoral global health governance.Adv Parasitol. 2021;114:1-26. doi: 10.1016/bs.apar.2021.08.007. Epub 2021 Oct 11. Adv Parasitol. 2021. PMID: 34696842 Free PMC article.
-
Efficacy and safety of ivermectin-albendazole combination versus ivermectin or albendazole monotherapy in soil-transmitted helminthiasis: A systematic review and meta-analysis.Medicine (Baltimore). 2025 Jan 17;104(3):e41280. doi: 10.1097/MD.0000000000041280. Medicine (Baltimore). 2025. PMID: 39833059 Free PMC article.
-
Egg excretion patterns of soil-transmitted helminth infections in humans following albendazole-ivermectin and albendazole treatment.PLoS Negl Trop Dis. 2024 Mar 22;18(3):e0012073. doi: 10.1371/journal.pntd.0012073. eCollection 2024 Mar. PLoS Negl Trop Dis. 2024. PMID: 38517907 Free PMC article. Clinical Trial.
-
Efficacy and safety of albendazole alone versus albendazole in combination with ivermectin for the treatment of Trichuris trichiura infections: An open-label, randomized controlled superiority trial in south-western Uganda.PLoS Negl Trop Dis. 2024 Nov 26;18(11):e0012687. doi: 10.1371/journal.pntd.0012687. eCollection 2024 Nov. PLoS Negl Trop Dis. 2024. PMID: 39591454 Free PMC article. Clinical Trial.
References
-
- WHO. Preventive chemotherapy in human helminthiasis - Coordinated use of anthelminthic drugs in control interventions: a manual for health professionals and programme managers. Geneva: World Health Organization; 2006.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
