

Long-Term Incidence of Stroke and Dementia in ASCOT
- PMID: 34192893
- PMCID: PMC8478091
- DOI: 10.1161/STROKEAHA.120.033489
Long-Term Incidence of Stroke and Dementia in ASCOT
Abstract
Background and purpose: Management of stroke risk factors might reduce later dementia. In ASCOT (Anglo-Scandinavian Outcome Trial), we determined whether dementia or stroke were associated with different blood pressure (BP)–lowering regimens; atorvastatin or placebo; and mean BP, BP variability, and mean cholesterol levels.
Methods: Participants with hypertension and ≥3 cardiovascular disease risk factors were randomly allocated to amlodipine- or atenolol-based BP-lowering regimen targeting BP <140/90 mm Hg for 5.5 years. Participants with total cholesterol ≤6.5 mmol/L were also randomly allocated to atorvastatin 10 mg or placebo for 3.3 years. Mean and LDL (low-density lipoprotein) cholesterol, BP, and SD of BP were calculated from 6 months to end of trial. UK participants were linked to electronic health records to ascertain deaths and hospitalization in general and mental health hospitals. Dementia and stroke were ascertained by validated code lists and within-trial ascertainment.
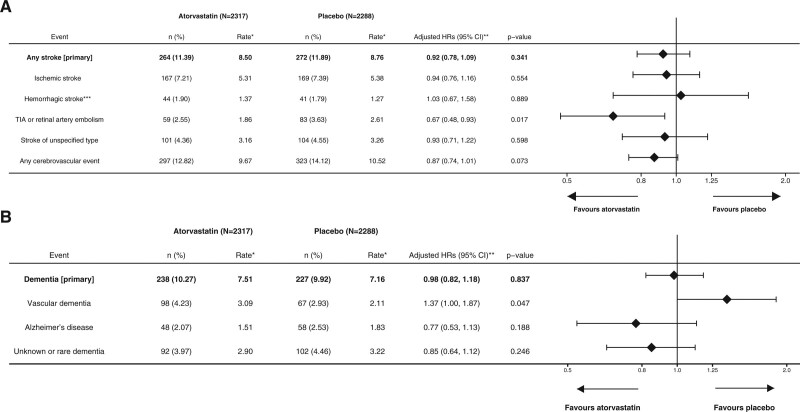
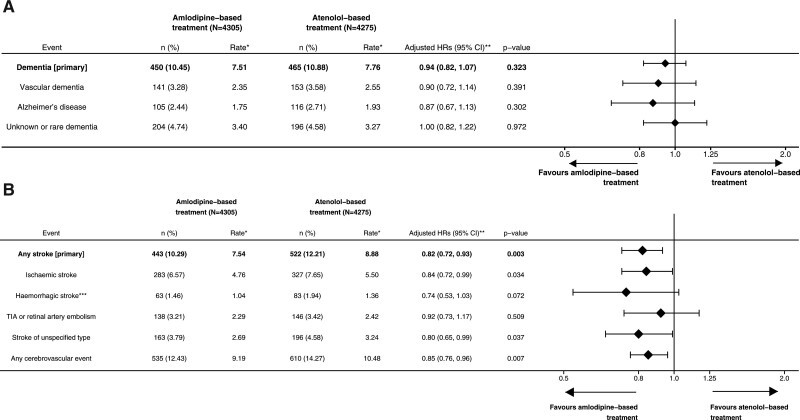
Results: Of 8580 UK participants, 7300 were followed up to 21 years from randomization. Atorvastatin for 3.3 years had no measurable effect on stroke (264 versus 272; adjusted hazard ratio [HR], 0.92 [95% CI, 0.78–1.09]; P=0.341) or dementia (238 versus 227; adjusted HR, 0.98 [95% CI, 0.82–1.18]; P=0.837) compared with placebo. Mean total cholesterol was not associated with later stroke or dementia. An amlodipine-based compared with an atenolol-based regimen for 5.5 years reduced stroke (443 versus 522; adjusted HR, 0.82 [95% CI, 0.72–0.93]; P=0.003) but not dementia (450 versus 465; adjusted HR, 0.94 [95% CI, 0.82–1.07]; P=0.334) over follow-up. BP variability (SD mean BP) was associated with a higher risk of dementia (per 5 mm Hg HR, 1.14 [95% CI, 1.06–1.24]; P<0.001) and stroke (HR, 1.21 [95% CI, 1.12–1.32]; P<0.001) adjusted for mean BP.
Conclusions: An amlodipine-based BP regimen reduced the long-term incidence of stroke compared with an atenolol-based regimen but had no measurable effect on dementia. Atorvastatin had no effect on either stroke or dementia. Higher BP variability was associated with a higher incidence of later dementia and stroke.
Keywords: blood pressure; cholesterol; dementia; risk factors; stroke.
Figures

Similar articles
-
Long-term mortality after blood pressure-lowering and lipid-lowering treatment in patients with hypertension in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Legacy study: 16-year follow-up results of a randomised factorial trial.Lancet. 2018 Sep 29;392(10153):1127-1137. doi: 10.1016/S0140-6736(18)31776-8. Epub 2018 Aug 26. Lancet. 2018. PMID: 30158072 Clinical Trial.
-
Antihypertensive therapy and the benefits of atorvastatin in the Anglo-Scandinavian Cardiac Outcomes Trial: lipid-lowering arm extension.J Hypertens. 2009 May;27(5):947-54. doi: 10.1097/HJH.0b013e328326cb1a. J Hypertens. 2009. PMID: 19318984
-
Potential synergy between lipid-lowering and blood-pressure-lowering in the Anglo-Scandinavian Cardiac Outcomes Trial.Eur Heart J. 2006 Dec;27(24):2982-8. doi: 10.1093/eurheartj/ehl403. Epub 2006 Dec 4. Eur Heart J. 2006. PMID: 17145722 Clinical Trial.
-
Amlodipine/Atorvastatin: a review of its use in the treatment of hypertension and dyslipidaemia and the prevention of cardiovascular disease.Drugs. 2010;70(2):191-213. doi: 10.2165/11204420-000000000-00000. Drugs. 2010. PMID: 20108992 Review.
-
The ASCOT trial: clarifying the role of ACE inhibition in the reduction of cardiovascular events in patients with hypertension.Am J Cardiovasc Drugs. 2006;6(5):327-34. doi: 10.2165/00129784-200606050-00005. Am J Cardiovasc Drugs. 2006. PMID: 17083267 Review.
Cited by
-
Antiplatelet therapy and incident cognitive impairment or dementia-a systematic review and meta-analysis of randomised clinical trials.Age Ageing. 2023 Oct 2;52(10):afad197. doi: 10.1093/ageing/afad197. Age Ageing. 2023. PMID: 37897809 Free PMC article.
-
The relationship of baseline high-sensitivity C-reactive protein with incident cardiovascular events and all-cause mortality over 20 years.EBioMedicine. 2025 Jul;117:105786. doi: 10.1016/j.ebiom.2025.105786. Epub 2025 Jun 4. EBioMedicine. 2025. PMID: 40472800 Free PMC article. Clinical Trial.
-
Comparative effects of angiotensin II stimulating and inhibiting antihypertensives on dementia risk: a systematic review and meta-analysis.Geroscience. 2025 Apr 4. doi: 10.1007/s11357-025-01600-1. Online ahead of print. Geroscience. 2025. PMID: 40183864 Review.
-
Assessing Risk Factors for Cognitive Decline Using Electronic Health Record Data: A Scoping Review.Res Sq [Preprint]. 2024 Aug 9:rs.3.rs-4671544. doi: 10.21203/rs.3.rs-4671544/v1. Res Sq. 2024. PMID: 39149490 Free PMC article. Preprint.
-
Comparing the predictive value of quantitative magnetic resonance imaging parametric response mapping and conventional perfusion magnetic resonance imaging for clinical outcomes in patients with chronic ischemic stroke.Front Neurosci. 2023 May 25;17:1177044. doi: 10.3389/fnins.2023.1177044. eCollection 2023. Front Neurosci. 2023. Retraction in: Front Neurosci. 2024 Oct 07;18:1504798. doi: 10.3389/fnins.2024.1504798. PMID: 37304032 Free PMC article. Retracted.
References
-
- Lincoln P, Fenton K, Alessi C, Prince M, Brayne C, Wortmann M, Patel K, Deanfield J, Mwatsama M. The blackfriars consensus on brain health and dementia. Lancet. 2014; 383:1805–1806. doi: 10.1016/S0140-6736(14)60758-3 - PubMed
-
- Fulcher J, O’Connell R, Voysey M, Emberson J, Blackwell L, Mihaylova B, Simes J, Collins R, Kirby A, Colhoun H, et al. . Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174 000 participants in 27 randomised trials. Lancet. 2015; 385:1397–1405 - PubMed
-
- Turnbull F; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2003; 362:1527–1535. doi: 10.1016/s0140-6736(03)14739-3 - PubMed
-
- Sever PS, Dahlöf B, Poulter NR, Wedel H, Beevers G, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, et al. ; ASCOT Investigators. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial–Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003; 361:1149–1158. doi: 10.1016/S0140-6736(03)12948-0 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
