

Monocyte distribution width (MDW) performance as an early sepsis indicator in the emergency department: comparison with CRP and procalcitonin in a multicenter international European prospective study
- PMID: 34193208
- PMCID: PMC8247285
- DOI: 10.1186/s13054-021-03622-5
Monocyte distribution width (MDW) performance as an early sepsis indicator in the emergency department: comparison with CRP and procalcitonin in a multicenter international European prospective study
Abstract
Background: Early sepsis diagnosis has emerged as one of the main challenges in the emergency room. Measurement of sepsis biomarkers is largely used in current practice to improve the diagnosis accuracy. Monocyte distribution width (MDW) is a recent new sepsis biomarker, available as part of the complete blood count with differential. The objective was to evaluate the performance of MDW for the detection of sepsis in the emergency department (ED) and to compare to procalcitonin (PCT) and C-reactive protein (CRP).
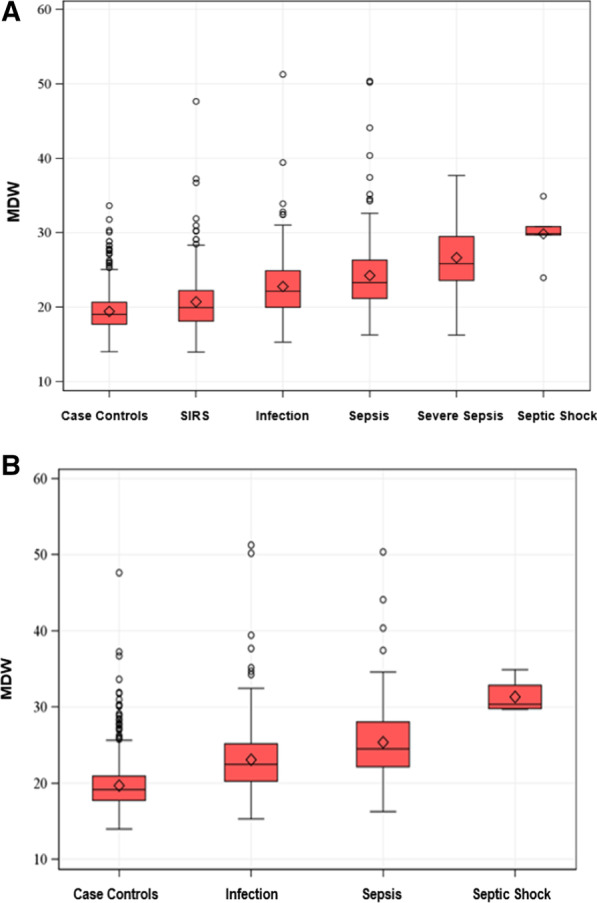
Methods: Subjects whose initial evaluation included a complete blood count were enrolled consecutively in 2 EDs in France and Spain and categorized per Sepsis-2 and Sepsis-3 criteria. The performance of MDW for sepsis detection was compared to that of procalcitonin (PCT) and C-reactive protein (CRP).
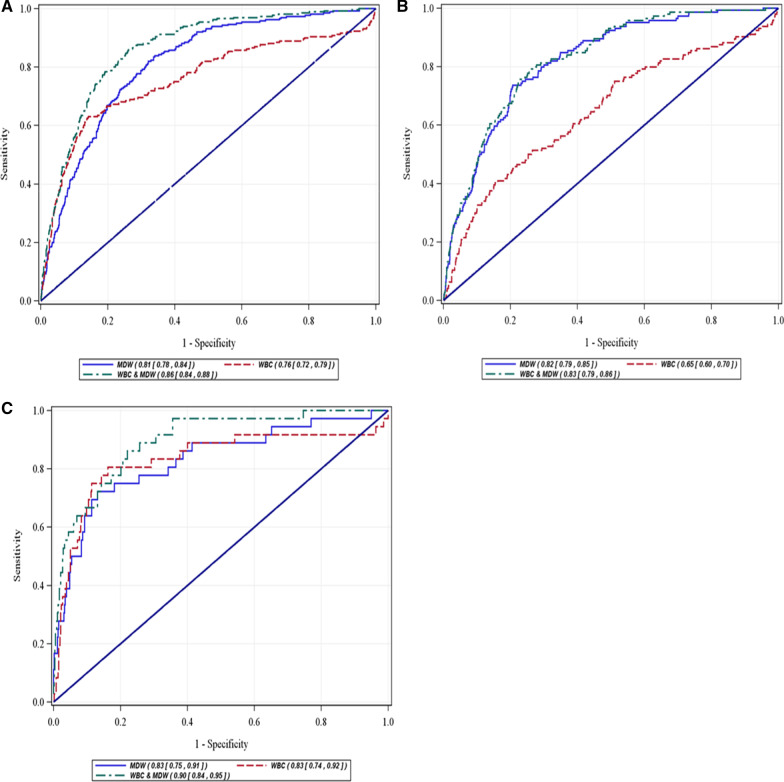
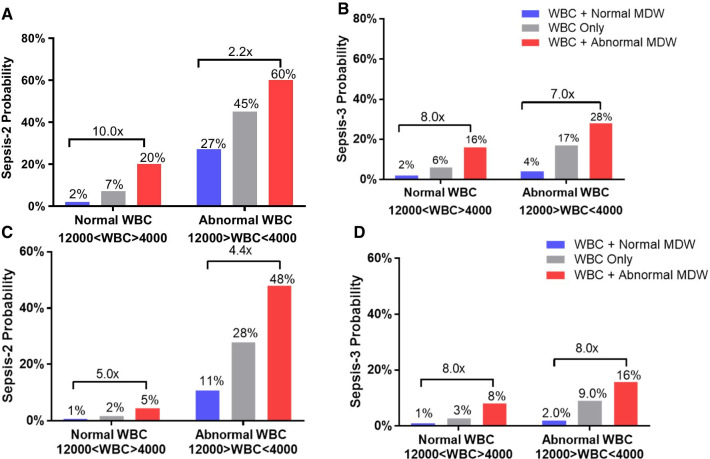
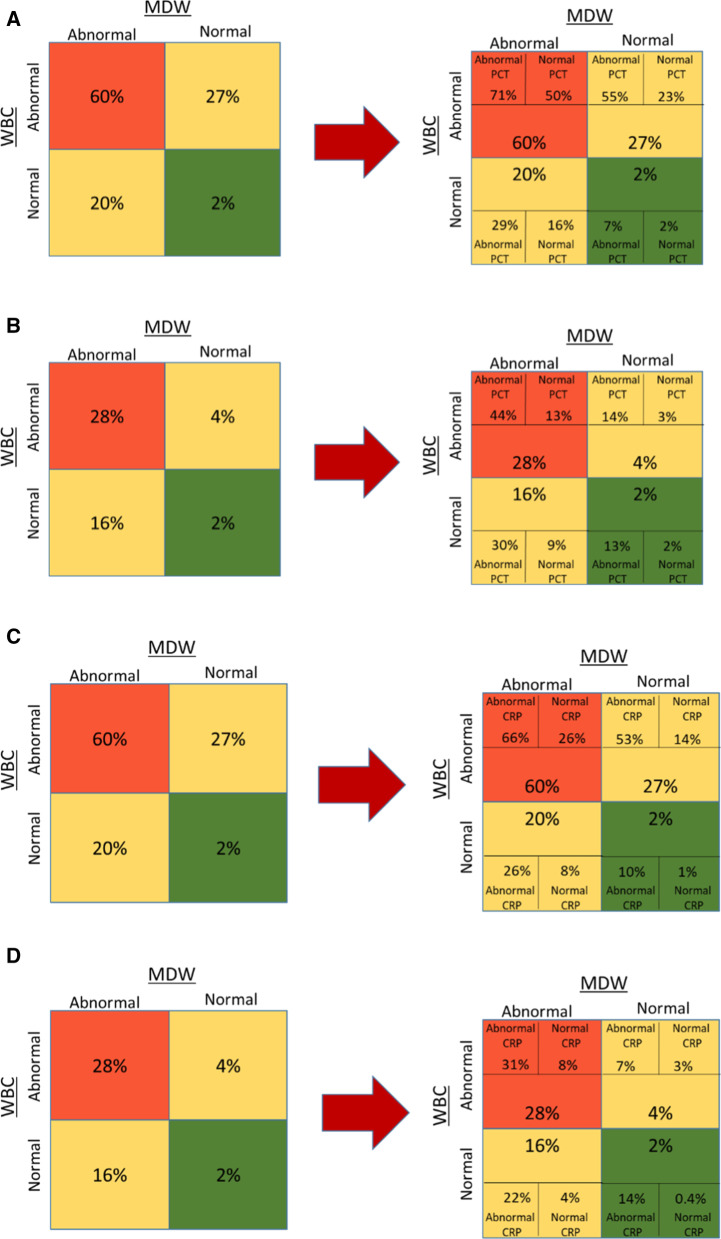
Results: A total of 1,517 patients were analyzed: 837 men and 680 women, mean age 61 ± 19 years, 260 (17.1%) categorized as Sepsis-2 and 144 patients (9.5%) as Sepsis-3. The AUCs [95% confidence interval] for the diagnosis of Sepsis-2 were 0.81 [0.78-0.84] and 0.86 [0.84-0.88] for MDW and MDW combined with WBC, respectively. For Sepsis-3, MDW performance was 0.82 [0.79-0.85]. The performance of MDW combined with WBC for Sepsis-2 in a subgroup of patients with low sepsis pretest probability was 0.90 [0.84-0.95]. The AUC for sepsis detection using MDW combined with WBC was similar to CRP alone (0.85 [0.83-0.87]) and exceeded that of PCT. Combining the biomarkers did not improve the AUC. Compared to normal MDW, abnormal MDW increased the odds of Sepsis-2 by factor of 5.5 [4.2-7.1, 95% CI] and Sepsis-3 by 7.6 [5.1-11.3, 95% CI].
Conclusions: MDW in combination with WBC has the diagnostic accuracy to detect sepsis, particularly when assessed in patients with lower pretest sepsis probability. We suggest the use of MDW as a systematic screening test, used together with qSOFA score to improve the accuracy of sepsis diagnosis in the emergency department. Trial Registration ClinicalTrials.gov (NCT03588325).
Keywords: C-reactive protein; Emergency department; MDW; Monocyte volume distribution width; Procalcitonin; Sepsis.
Conflict of interest statement
PH receive consultant and advisory board fees from Beckman Coulter, educational support and congress communication fees from ThermoFisher Scientific, Radiometer and bioMérieux. IC, DC and LT are employed by Beckman Coulter, Inc., the sponsor of the clinical study. The other authors have no conflict of interest or competing interest to declare.
Figures

References
-
- EPISEPSIS: a reappraisal of the epidemiology and outcome of severe sepsis in French intensive care units. Intens Care Med. 2004;30(4):580–588. 10.1007/s00134-003-2121-4 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
