

Evaluation of different grafting materials for alveolar cleft repair in the context of orthodontic tooth movement in rats
- PMID: 34193933
- PMCID: PMC8245488
- DOI: 10.1038/s41598-021-93033-x
Evaluation of different grafting materials for alveolar cleft repair in the context of orthodontic tooth movement in rats
Abstract
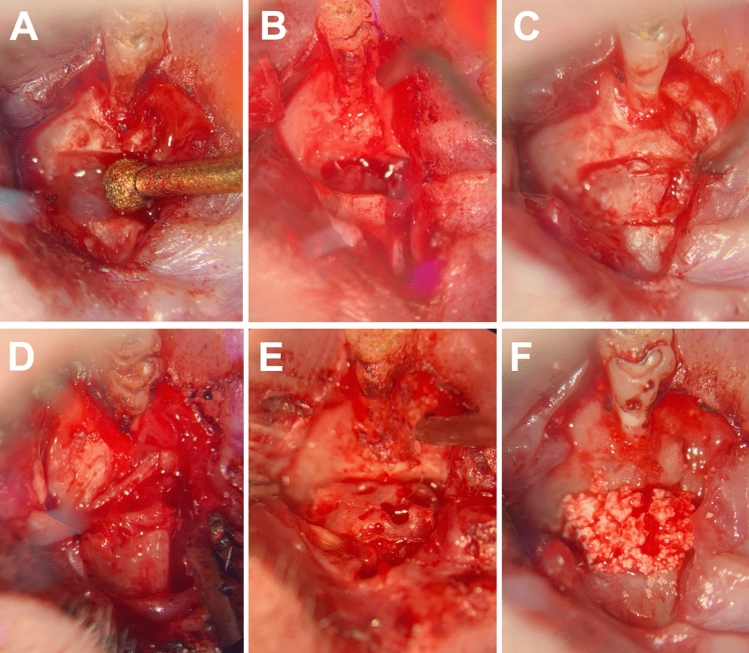
To minimize the postoperative risks posed by grafting autologous transplants for cleft repair, efforts are being made to improve grafting materials for use as potential alternatives. The aim of this study was to compare the bone graft quality of different bone substitutes including the gold standard autografts during the healing processes after cleft repair in the context of orthodontic treatment. In 21 Wistar rats, a complete, continuity-interrupting cleft was created. After 4 weeks, cleft repair was performed using autografts from the hips' ischial tuberosity, human xenografts, or synthetic bone substitutes [beta-tricalcium phosphate (β-TCP)/hydroxyapatite (HA)]. After another 4 weeks, the first molar movement was initiated in the reconstructed jaw for 8 weeks. The bone remodeling was analyzed in vivo using micro-computed tomography (bone mineral density and bone volume fraction) and histology (new bone formation). All the grafting materials were statistically different in bone morphology, which changed during the treatment period. The β-TCP/HA substitute demonstrated less resorption compared to the autologous and xenogeneic/human bone, and the autografts led to a stronger reaction in the surrounding bone. Histologically, the highest level of new bone formation was found in the human xenografts, and the lowest was found in the β-TCP/HA substitute. The differences between the two bone groups and the synthetic materials were statistically significant. Autografts were confirmed to be the gold standard in cleft repair with regard to graft integration. However, parts of the human xenograft seemed comparable to the autografts. Thus, this substitute could perhaps be used as an alternative after additional tissue-engineered modification.
Conflict of interest statement
The authors declare no competing interests.
Figures








References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
