

Treatment of ARS deficiencies with specific amino acids
- PMID: 34194004
- PMCID: PMC8244667
- DOI: 10.1038/s41436-021-01249-z
Treatment of ARS deficiencies with specific amino acids
Abstract
Purpose: Recessive cytosolic aminoacyl-tRNA synthetase (ARS) deficiencies are severe multiorgan diseases, with limited treatment options. By loading transfer RNAs (tRNAs) with their cognate amino acids, ARS are essential for protein translation. However, it remains unknown why ARS deficiencies lead to specific symptoms, especially early life and during infections. We set out to increase pathophysiological insight and improve therapeutic possibilities.
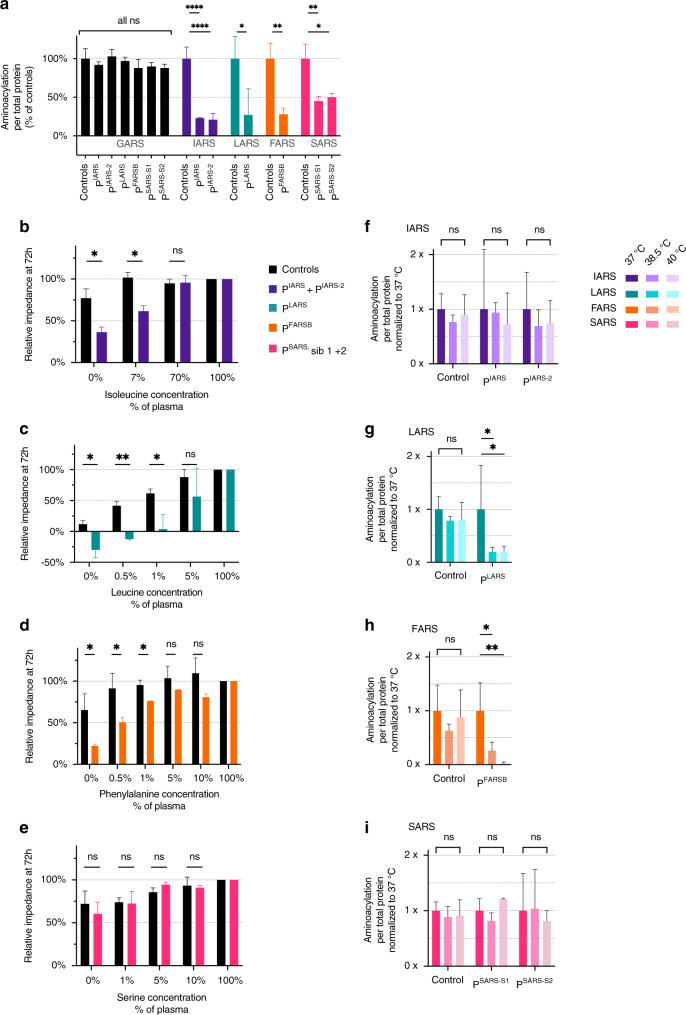
Methods: In fibroblasts from patients with isoleucyl-RS (IARS), leucyl-RS (LARS), phenylalanyl-RS-beta-subunit (FARSB), and seryl-RS (SARS) deficiencies, we investigated aminoacylation activity, thermostability, and sensitivity to ARS-specific amino acid concentrations, and developed personalized treatments.
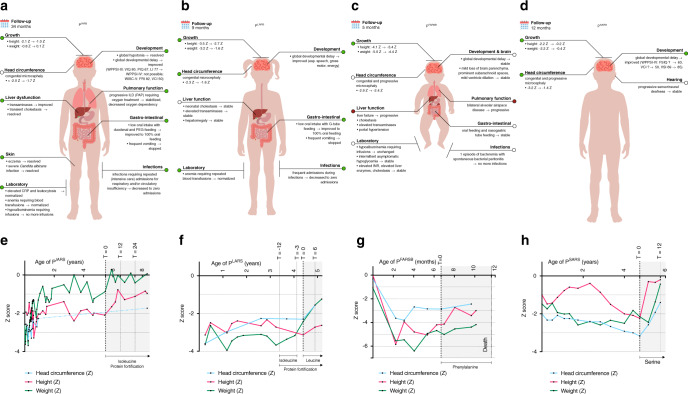
Results: Aminoacylation activity was reduced in all patients, and further diminished at 38.5/40 °C (PLARS and PFARSB), consistent with infectious deteriorations. With lower cognate amino acid concentrations, patient fibroblast growth was severely affected. To prevent local and/or temporal deficiencies, we treated patients with corresponding amino acids (follow-up: 1/2-2 2/3rd years), and intensified treatment during infections. All patients showed beneficial treatment effects, most strikingly in growth (without tube feeding), head circumference, development, coping with infections, and oxygen dependency.
Conclusion: For these four ARS deficiencies, we observed a common disease mechanism of episodic insufficient aminoacylation to meet translational demands and illustrate the power of amino acid supplementation for the expanding ARS patient group. Moreover, we provide a strategy for personalized preclinical functional evaluation.
© 2021. The Author(s), under exclusive licence to the American College of Medical Genetics and Genomics.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Correspondence on "Treatment of ARS deficiencies with specific amino acids" by Kok et al.Genet Med. 2022 Feb;24(2):503-505. doi: 10.1016/j.gim.2021.10.001. Epub 2021 Nov 30. Genet Med. 2022. PMID: 34906482 No abstract available.
-
Response to Shen et al.Genet Med. 2022 Feb;24(2):506-507. doi: 10.1016/j.gim.2021.09.022. Epub 2021 Nov 30. Genet Med. 2022. PMID: 34906483 No abstract available.
References
-
- Antonellis A, Green ED. The role of aminoacyl-tRNA synthetases in genetic diseases. Annu Rev Genomics Hum Genet 2008;9:87–107. - PubMed
-
- Kraulis PJ. MOLSCRIPT: a program to produce both detailed and schematic plots of protein structures. J Appl Crystallogr. 1991;24:947–50. doi: 10.1107/S0021889891004399. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
