

The Role of Oxidative Stress in Hypertensive Disorders of Pregnancy (Preeclampsia, Gestational Hypertension) and Metabolic Disorder of Pregnancy (Gestational Diabetes Mellitus)
- PMID: 34194606
- PMCID: PMC8184326
- DOI: 10.1155/2021/5581570
The Role of Oxidative Stress in Hypertensive Disorders of Pregnancy (Preeclampsia, Gestational Hypertension) and Metabolic Disorder of Pregnancy (Gestational Diabetes Mellitus)
Abstract
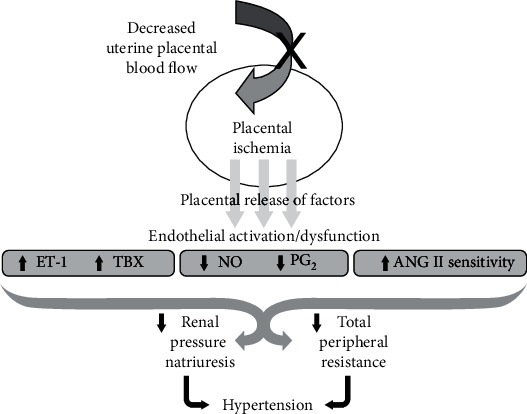
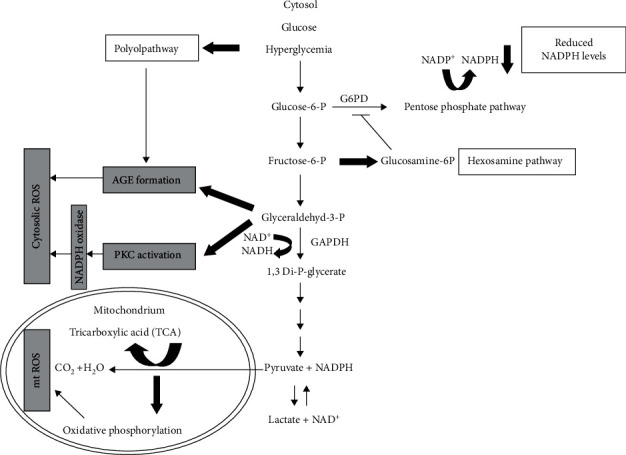
Purpose of the Review.To highlight the role of oxidative stress in hypertensive disorders of pregnancy (HDP) and metabolic disorders of pregnancy (gestational diabetes mellitus). Recent Findings. In both preeclampsia (PE) and gestational hypertension (GH), oxidative stress leads to inadequate placental perfusion thus resulting in a hypoxic placenta, which generally leads to the activation of maternal systemic inflammatory response. In PE, this causes inflammation in the kidneys and leads to proteinuria. A proteinuria marker known as urinary 8-oxoGuo excretion is expressed in preeclampsia. In GDM, oxidative stress plays a role in the pathogenesis of the disease, as a result of over secretion of insulin during pregnancy. This uncontrolled secretion of insulin results in the production of lipid peroxidation factors that also mask the secretion of antioxidants. Therefore, ROS becomes abundant at cellular level and prevents the cells from transporting glucose to body tissues. Summary. There is a need for more research investigating the role of oxidative stress, especially in obstetrics-related conditions. More studies are required in order to understand the difference between the pathogenesis and pathophysiology of PE versus GH since investigations on the differences in genetic aspects of each condition are lacking. Furthermore, research to improve diagnostic procedures for GDM in pregnancy is needed.
Copyright © 2021 Wendy N. Phoswa and Olive P. Khaliq.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Duley L. The global impact of pre-eclampsia and eclampsia. Seminars in perinatology. Elsevier; 2009. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
