

A Novel guide extension assisted stenting technique for coronary bifurcation lesions
- PMID: 34194633
- PMCID: PMC8223698
- DOI: 10.4330/wjc.v13.i6.155
A Novel guide extension assisted stenting technique for coronary bifurcation lesions
Abstract
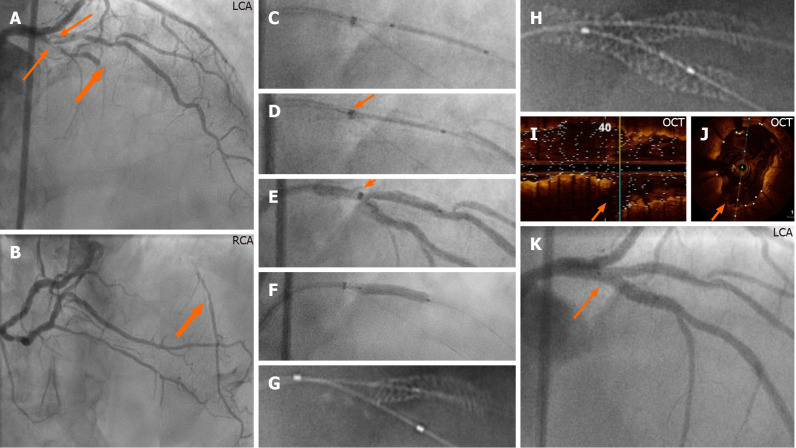
A challenging technical scenario frequently encountered in a percutaneous coronary intervention of a coronary bifurcation lesion (CBL) is stent implantation of only the stenosed segment without compromising the other two normal segments in non-true bifurcation lesions. Another is precise stent implantation covering the side branch ostium without leaving excessive stent metal at the other two segments of a bifurcation lesion in complex true bifurcation lesions. The aim of this study was to describe a novel stenting technique for both non-true and true CBLs by using a guide extension catheter (GuideLiner). With the assistance of a guide extension catheter mounted on both the main and the side-branch guidewires and with its intubation down to the bifurcation carina, a stent can be implanted in the side branch segment or distal main segment of the bifurcation lesion appropriately without compromising the other two segments of the coronary bifurcation. Stent implantation is described in three bifurcation lesions in three cases and shown in detail with illustrative figures. The technique facilitates side-branch only stenting in side-branch mono-ostial (medina 0, 0, 1) CBL or only the distal main segment in distal mono-ostial (medina 0, 1, 0) CBL without compromising the other two remaining segments when using the one-stent technique in non-true CBLs without leaving unnecessary excessive stent metal at the bifurcation site and when using a two-stent technique in complex true bifurcation lesions (tri-ostial or medina 1, 1, 1). Consequently, through optimizing stent deployment, the technique may have the potential to reduce the risk of subacute stent thrombosis and future in-stent restenosis. The most appropriate lesions suitable for the technique, and some other practical tips are also described.
Keywords: Coronary bifurcation lesion; GuideLiner stenting; Medina classification; Novel descriptive, intelligible and ordered classification; One- or two-stenting technique; Percutaneous coronary intervention.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no competing interests to disclose.
Figures



Similar articles
-
True coronary bifurcation lesions: meta-analysis and review of literature.J Cardiovasc Med (Hagerstown). 2010 Feb;11(2):103-10. doi: 10.2459/JCM.0b013e32832ffc85. J Cardiovasc Med (Hagerstown). 2010. PMID: 19952947 Review.
-
Modified T-stenting with intentional protrusion of the side-branch stent within the main vessel stent to ensure ostial coverage and facilitate final kissing balloon: the T-stenting and small protrusion technique (TAP-stenting). Report of bench testing and first clinical Italian-Korean two-centre experience.Catheter Cardiovasc Interv. 2007 Jul 1;70(1):75-82. doi: 10.1002/ccd.21194. Catheter Cardiovasc Interv. 2007. PMID: 17585382 Clinical Trial.
-
Stenting of bifurcation lesions: a rational approach.J Interv Cardiol. 2001 Dec;14(6):573-85. doi: 10.1111/j.1540-8183.2001.tb00375.x. J Interv Cardiol. 2001. PMID: 12053378 Review.
-
Evaluation of a bifurcation drug-eluting stent system versus provisional T-stenting in a perfused synthetic coronary artery model.J Interv Cardiol. 2009 Dec;22(6):537-46. doi: 10.1111/j.1540-8183.2009.00509.x. Epub 2009 Nov 13. J Interv Cardiol. 2009. PMID: 19912465
-
Double Kissing Crush Versus Provisional Stenting for Left Main Distal Bifurcation Lesions: DKCRUSH-V Randomized Trial.J Am Coll Cardiol. 2017 Nov 28;70(21):2605-2617. doi: 10.1016/j.jacc.2017.09.1066. Epub 2017 Oct 30. J Am Coll Cardiol. 2017. PMID: 29096915 Clinical Trial.
Cited by
-
Drug-Eluting Balloons Versus Conventional Balloons in Treatment of Coronary Bifurcation Lesions in Small Vessels.Med Sci Monit. 2025 Jul 17;31:e948370. doi: 10.12659/MSM.948370. Med Sci Monit. 2025. PMID: 40671280 Free PMC article.
-
Guide Extension-Facilitated Ostial Stenting (GEST) During Primary Coronary Angioplasty in a Patient With ST-Segment Elevation Myocardial Infarction: A Case Report.Cureus. 2024 Dec 5;16(12):e75148. doi: 10.7759/cureus.75148. eCollection 2024 Dec. Cureus. 2024. PMID: 39764315 Free PMC article.
References
-
- Collet C, Mizukami T, Grundeken MJ. Contemporary techniques in percutaneous coronary intervention for bifurcation lesions. Expert Rev Cardiovasc Ther. 2018;16:725–734. - PubMed
-
- Y-Hassan S, Lindroos MC, Sylvén C. A novel stenting technique for coronary artery bifurcation stenosis. Catheter Cardiovasc Interv. 2009;73:903–909. - PubMed
-
- Y-Hassan S, Lindroos MC, Sylvén C. A Novel Descriptive, Intelligible and Ordered (DINO) classification of coronary bifurcation lesions. Review of current classifications. Circ J. 2011;75:299–305. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
