

Surgical Treatment of Intramuscular Myxoma
- PMID: 34194644
- PMCID: PMC8192669
- DOI: 10.1007/s43465-021-00367-9
Surgical Treatment of Intramuscular Myxoma
Abstract
Purpose: Intramuscular myxoma (IM) is a rare benign myxoid tumor that may be challenging to differentiate from sarcoma in small amounts of biopsied material. Although IM appears to be well-circumscribed macroscopically, it infiltrates the adjacent edematous muscle microscopically. The recommended treatment is resection, but there is controversy with regard to the appropriate surgical margin. This study aimed to clarify which surgical procedure that should be applied when the preoperative diagnosis is IM and how to manage treatment if the postoperative diagnosis turns out to be a sarcoma.
Methods: We retrospectively examined 55 IM patients treated from January 1982 to December 2014. Patient characteristics, tumor location, tumor size, radiograph, preoperative and postoperative pathological reports, surgical techniques, treatment outcome, and complications were reviewed. The patients were followed up on for at least 5 years. All patients were confirmed not to have Mazabraud syndrome.
Results: In the 55 IM patients examined, the mean patient age was 48 years and most were female. The most common tumor locations were in the muscles of the thighs (47%) and buttocks (20%). The mean tumor diameter was 5 cm. Wide resection and marginal resection were performed in 24 and 31 patients, respectively. The mean follow-up duration was 19 years. No local recurrence, malignant transformation, or complications were observed.
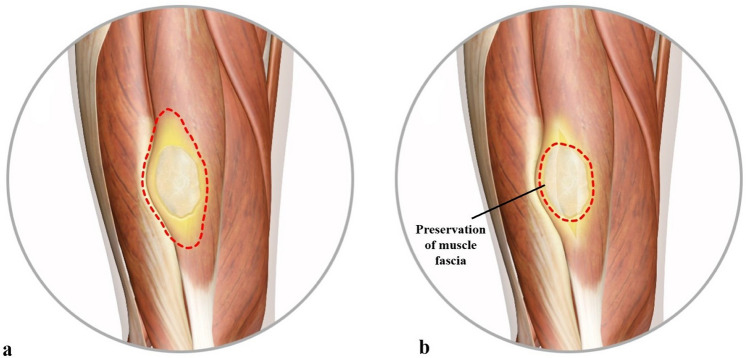
Conclusions: Marginal resection is suitable in patients whose preoperative diagnosis is IM, as it is able to prevent local recurrence and allows for the preservation of muscle and muscle fascia. If the postoperative diagnosis turns out to be myxoid sarcoma, minimum surgical contamination makes additional wide resection less invasive.
Keywords: Inadvertent resection; Intramuscular myxoma; Marginal resection; Wide resection.
© Indian Orthopaedics Association 2021.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflict of interest.
Figures


References
-
- Gaumetou E, Tomeno B, Anract P. Mazabraud’s syndrome. A case with multiple myxomas. Orthopaedics & Traumatology: Surgery. 2012;98:455–460. - PubMed
LinkOut - more resources
Full Text Sources