

A Surgical Protocol for Management of Post Traumatic Heterotopic Ossification of Elbow
- PMID: 34194645
- PMCID: PMC8192647
- DOI: 10.1007/s43465-021-00381-x
A Surgical Protocol for Management of Post Traumatic Heterotopic Ossification of Elbow
Abstract
Background: Open excision remains the gold standard of treatment for posttraumatic heterotopic ossification (HO) of the elbow. The purpose of this study is to evaluate the functional outcome of early surgical excision done by adhering to a proposed surgical protocol with exclusive posttraumatic HO of the elbow.
Methods: A retrospective study was conducted with 31 patients (25 males and 6 females) with a mean follow-up of 40.5 ± 27.44 months. Excision was done according to our surgical protocol based on the location of HO, associated fractures, stability, need for ulnar nerve transposition, previous operative scar. Improvement in elbow function, Mayo elbow performance score (MEPS) preoperatively and at final follow-up was compared, and statistical analysis was done.
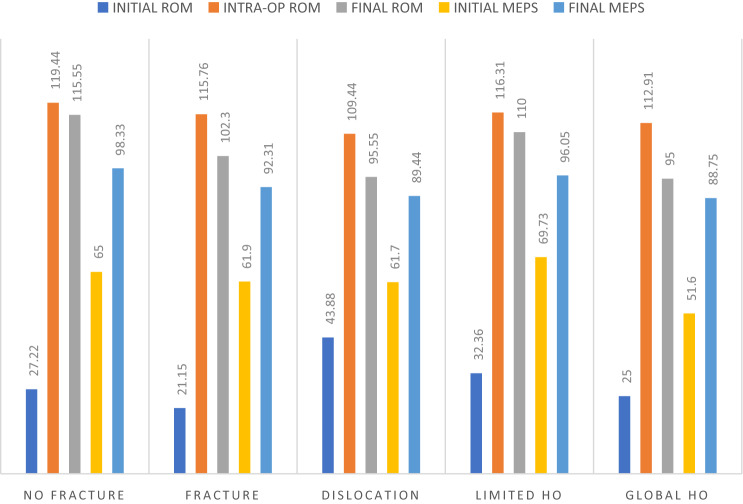
Results: Mean flexion-extension arc, supination-pronation arc and MEPS improved by 74.68° ± 29.32°, 26.13° ± 32.93°, 30.48 ± 11.57, respectively. Flexion arc deteriorated by 10.81° ± 10.42° from intraoperative to final follow-up. Improvement at final follow-up was significant in all the cases (P < 0.05). 19 patients had limited HO, and 12 had global HO. Their mean flexion-extension arc increase was 77.63° ± 29.12° and 70° ± 30.3° respectively, and the final mean MEPS score was 96.05 ± 5.16 and 88.75 ± 11.51, respectively. Nine patients had no initial fracture (Group 1), 13 had some fracture (Group 2), nine had a fracture-dislocation of the elbow (Group 3). Their flexion-extension improvement, final MEPS were 88.33° ± 30.82°, 98.33 ± 5, (Group 1); 81.15° ± 16.73°, 92.31 ± 9.27 (Group 2) and 51.67° ± 31.32°, 89.44 ± 9.5 (Group 3), respectively. We had two complications (6.45%).
Conclusion: The surgical protocol described here enabled us to achieve good functional results and was in concordance with similar studies done previously.
Supplementary information: The online version contains supplementary material available at 10.1007/s43465-021-00381-x.
Keywords: Elbow stiffness; HO excision; Heterotopic ossification; Surgical protocol.
© Indian Orthopaedics Association 2021.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflict of interest related to this work.
Figures

References
-
- Morrey, B. F., & Sanchez-Sotelo, J. (2010). The elbow and its disorders, 4th edn. In Morrey, B., & Sanchez-Sotelo, J. (Eds.) Bone (p. 472–483).
-
- Morrey BF, An K-N. Functional evaluation of the elbow. In: Morrey BF, editor. The elbow and its disorders. 4. Philadelphia: Elsevier; 2008. p. 88.
LinkOut - more resources
Full Text Sources