

Accuracy in the Execution of Pre-operative Plan for Limb Alignment and Implant Positioning in Robotic-arm Assisted Total Knee Arthroplasty and Manual Total Knee Arthroplasty: A Prospective Observational Study
- PMID: 34194653
- PMCID: PMC8192671
- DOI: 10.1007/s43465-020-00324-y
Accuracy in the Execution of Pre-operative Plan for Limb Alignment and Implant Positioning in Robotic-arm Assisted Total Knee Arthroplasty and Manual Total Knee Arthroplasty: A Prospective Observational Study
Abstract
Aim: The objective of the study is to compare the accuracy of implant positioning and limb alignment achieved in robotic-arm assisted total knee arthroplasty(RATKA) and manual total knee arthroplasty(MTKA) to their respective preoperative plan.
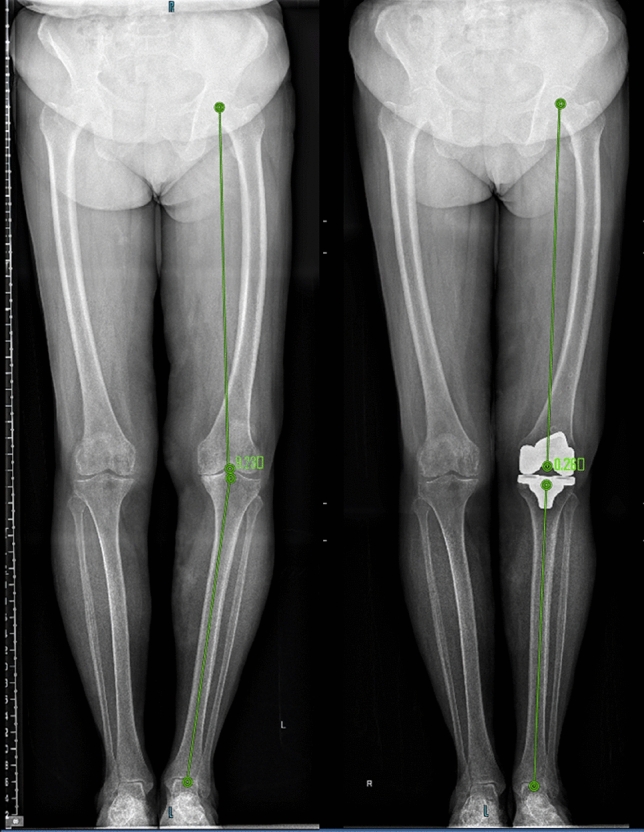
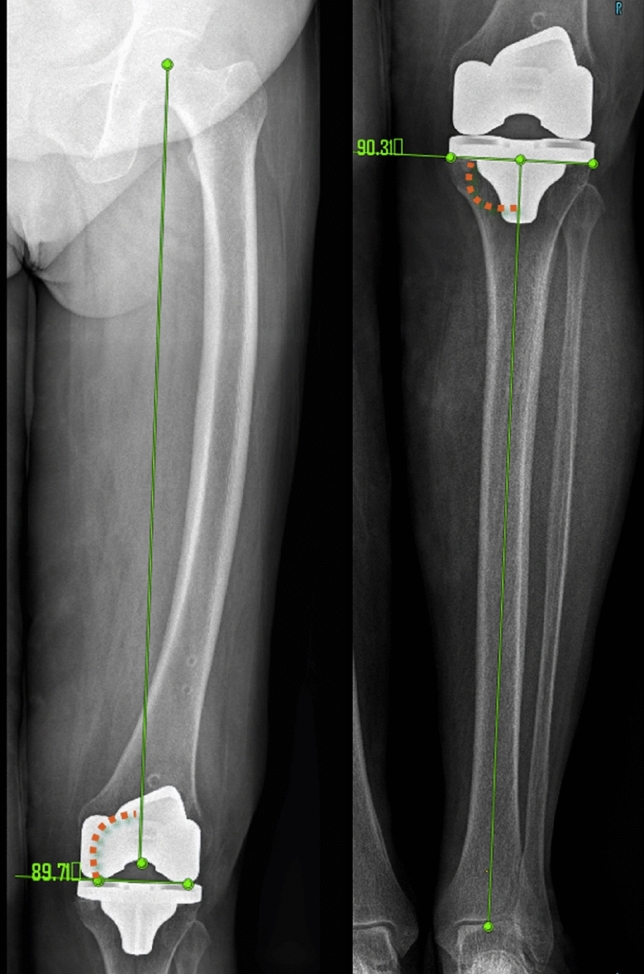
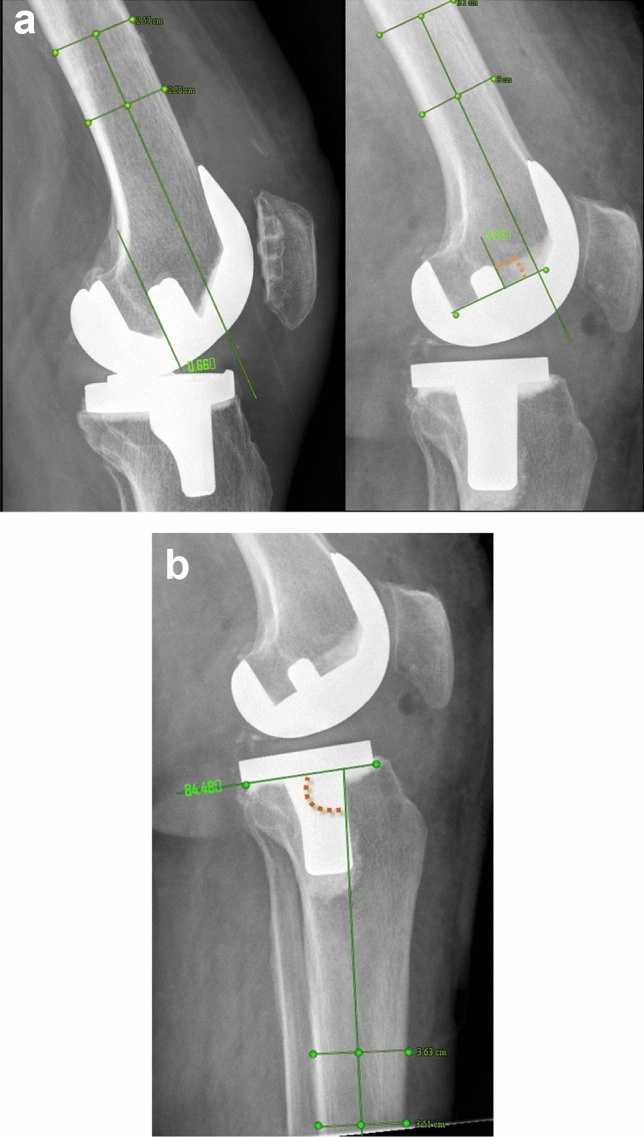
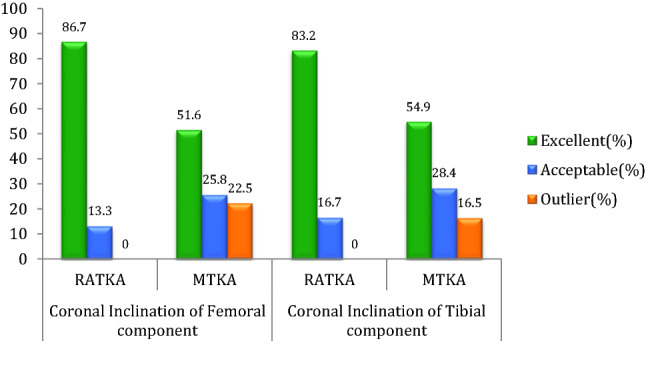
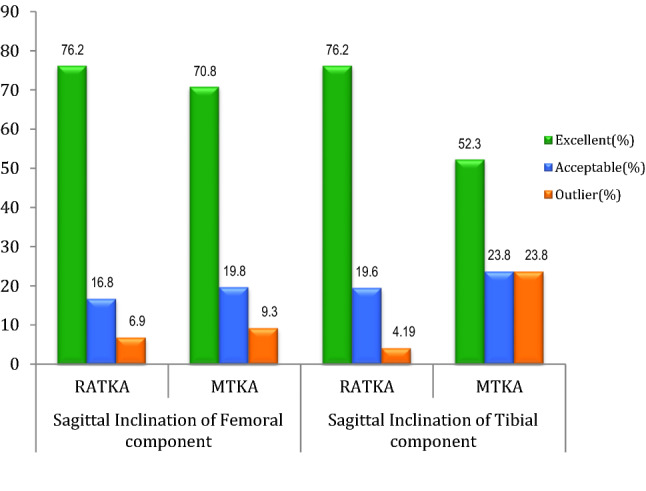
Patients and methods: This was a prospective observational study conducted in a tertiary care centre between August 2018 and January 2020. 143 consecutive RATKA(105 patients) and 151 consecutive MTKA(111 patients) performed by two experienced arthroplasty surgeons were included. Two independent observers evaluated the accuracy of implant positioning by measuring the radiological parameters according to the Knee-Society-Roentgenographic-Evaluation-System and limb alignment from postoperative weight-bearing scanogram. Outcomes were defined, based on the degree of deviation of measurements from the planned position and alignment, as excellent(0-1.99°), acceptable(2.00-2.99°) and outlier(≥ 3.00°).
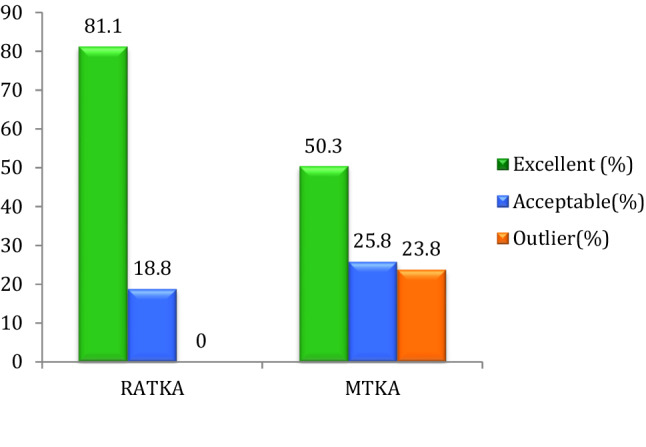
Results: There were no systematic differences in the demographic and baseline characteristics between RATKA and MTKA. Statistically significant outcomes were observed favouring robotic group for postoperative mechanical axis (p < .001), coronal inclination of the femoral component (p < 0.001), coronal inclination of tibial component (p < 0.001), and sagittal inclination of tibial component (p < 0.001). There was no significant difference in the sagittal inclination of the femoral component (p = 0.566). The percentage of knees in the 'excellent' group were higher in RATKA compared to MTKA. There was absolutely no outlier in terms of limb alignment in the RATKA group versus 23.8% (p < 0.001) in the MTKA group. All the measurements showed high interobserver and intraobserver reliability.
Conclusion: Robotic-arm assisted TKA executed the preoperative plan more accurately with respect to limb alignment and implant positioning compared to manual TKA, even when the surgeons were more experienced in the latter.
Supplementary information: The online version contains supplementary material available at 10.1007/s43465-020-00324-y.
Keywords: Accuracy; Arthroplasty; Implant position; Limb alignment; Manual; Osteoarthritis; Radiology; Robotic surgery; Robotic-arm assisted; Total knee arthroplasty.
© Indian Orthopaedics Association 2021.
Conflict of interest statement
Conflict of interestOn behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
References
-
- Gibon E, Goodman MJ, Goodman SB. Patient satisfaction after total knee arthroplasty: a realistic or imaginary goal? Orthopedic Clinics of North America. 2017;48(4):421–431. - PubMed
-
- Scott CEH, Turnbull GS, MacDonald D, Breusch SJ. Activity levels and return to work following total knee arthroplasty in patients under 65 years of age. Bone Joint J. 2017;99-B(8):1037–1046. - PubMed
-
- Luna IE, Kehlet H, Peterson B, Wede HR, Hoevsgaard SJ, Aasvang EK. Early patient-reported outcomes versus objective function after total hip and knee arthroplasty: a prospective cohort study. Bone Joint J. 2017;99-B(9):1167–1175. - PubMed
-
- Sikorski JM. Alignment in total knee replacement. Journal of Bone and Joint Surgery. British Volume. 2008;90(9):1121–1127. - PubMed
LinkOut - more resources
Full Text Sources