

Impact of primary medical or surgical therapy on prolactinoma patients' BMI and metabolic profile over the long-term
- PMID: 34195008
- PMCID: PMC8237353
- DOI: 10.1016/j.jcte.2021.100258
Impact of primary medical or surgical therapy on prolactinoma patients' BMI and metabolic profile over the long-term
Abstract
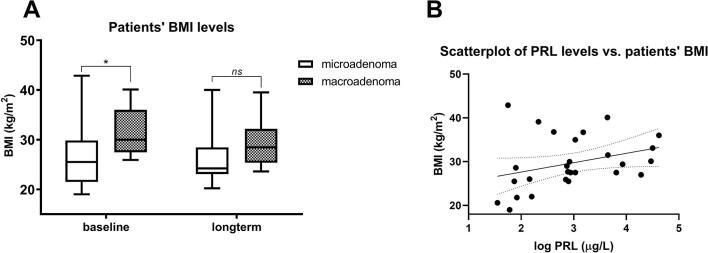
Objectives: High prolactin levels have been associated with weight gain and impaired metabolic profiles. While treatment with dopamine agonists (DAs) has been shown to improve these parameters, there is a lack of surgical series on its comparative effect in prolactinoma patients.
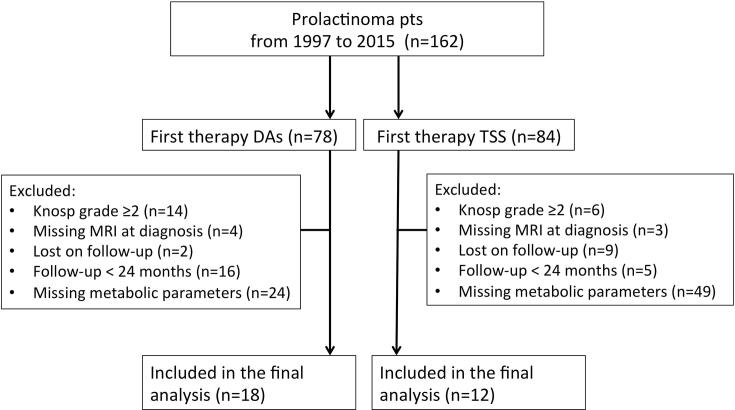
Methods: In this retrospective, comparative study, consecutive patients with a prolactinoma were enrolled if treated with first-line transsphenoidal surgery (TSS) or with DAs. Patients with prolactinomas of Knosp grade >2 and those with a follow-up <24 months were excluded, as were patients with missing laboratory metabolic parameters at baseline and over the long-term. Effects of either treatment on BMI and the metabolic profile were analyzed, and independent risk factors for long-term obesity were calculated.
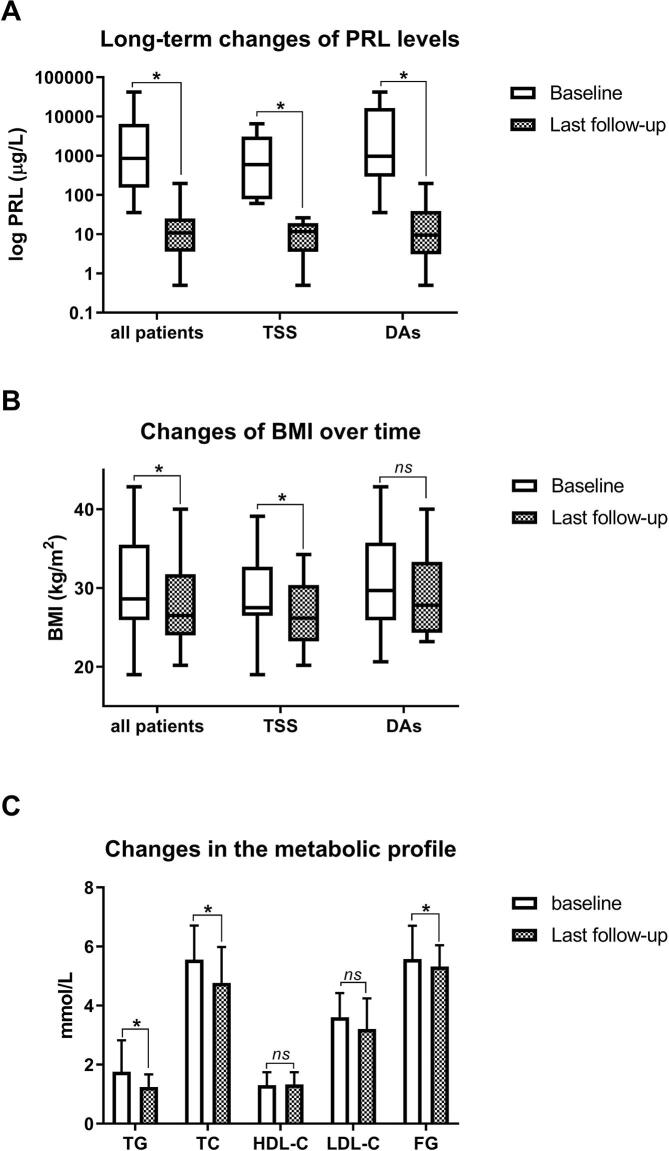
Results: Primary treatment was TSS for 12 patients (40%) and DAs for 18 patients (60%). At diagnosis, no significant differences between the two cohorts were observed with regard to adenoma size, Knosp grading, baseline prolactin (PRL) levels, prevalence of hypogonadism, or laboratory metabolic parameters. Mean follow-up was 51.9 months (range, 24-158). Over the long-term, both TSS and DAs led to the control of hyperprolactinemia (92% vs. 72%) and hypogonadism (78% vs. 83%) in the majority of patients. While a significant decrease in patients' BMI and fasting glucose were observed, changes in the lipid profile were marginal and independent of the treatment modality. At baseline, increased BMI-but not the primary treatment strategy-was an independent predictor of long-term obesity.
Conclusions: Over the long-term, patients' BMI and FG improve, but changes in the metabolic profile are marginal and independent of the primary treatment. It is presumable that not DAs per se, but rather the control of hyperprolactinemia plays a role in patients' metabolic profile alterations.
Keywords: BMI; Dopamine agonist; Metabolic profile; Prolactinoma; Surgery.
© 2021 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Wilding J.P.H. Endocrine testing in obesity. Eur J Endocrinol. 2020;182:C13–C15. - PubMed
-
- Shibli-Rahhal A., Schlechte J. The effects of hyperprolactinemia on bone and fat. Pituitary. 2009;12:96–104. - PubMed
-
- Raverot G., Jouanneau E., Trouillas J. Management of endocrine disease: clinicopathological classification and molecular markers of pituitary tumours for personalized therapeutic strategies. Eur J Endocrinol. 2014;170:R121–R132. - PubMed
