

Effect of β-blockers on the risk of COPD exacerbations according to indication of use: the Rotterdam Study
- PMID: 34195251
- PMCID: PMC8236616
- DOI: 10.1183/23120541.00624-2020
Effect of β-blockers on the risk of COPD exacerbations according to indication of use: the Rotterdam Study
Abstract
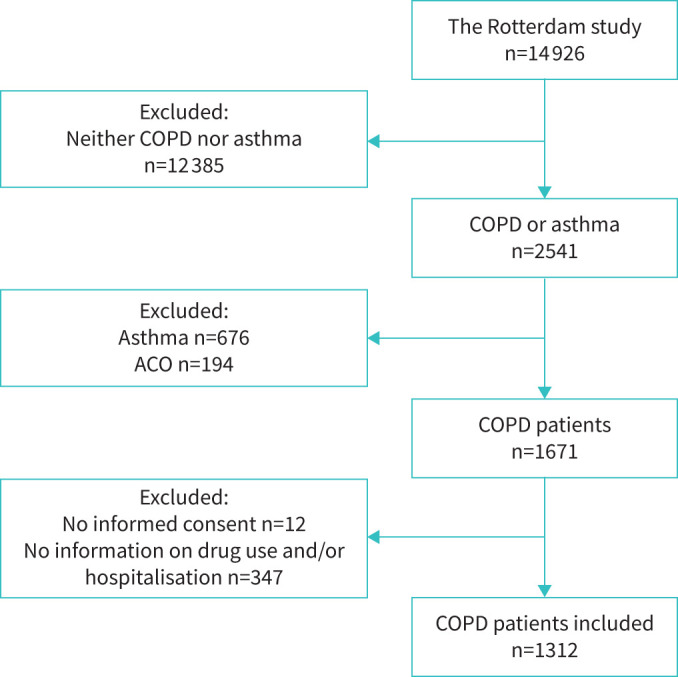
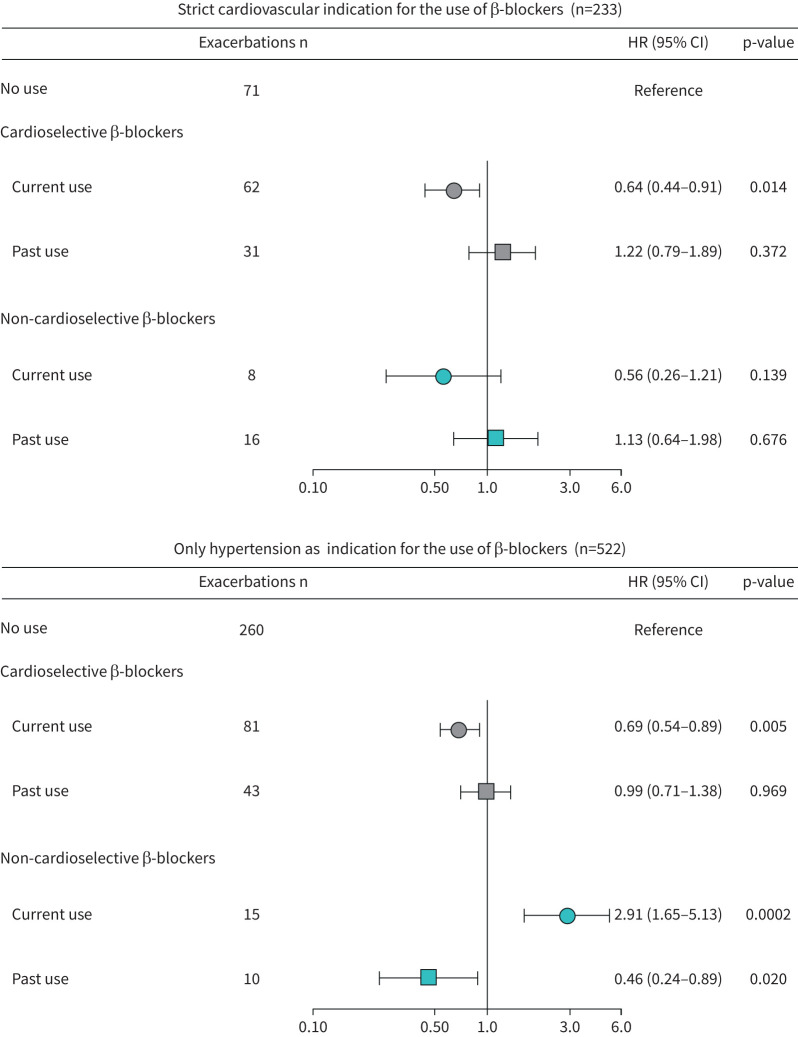
Observational studies report a reduction of COPD exacerbations in patients treated with β-blockers. In contrast, the Beta-Blockers for the Prevention of Acute Exacerbations of Chronic Obstructive Pulmonary Disease (BLOCK COPD) randomised controlled trial which excluded COPD patients with cardiovascular conditions showed an increase in COPD exacerbations. It is unclear whether this discrepancy could be explained by underlying cardiovascular comorbidity. We examined whether the association between use of β-blockers and risk of COPD exacerbations differed between patients with and without a cardiovascular indication for β-blockers use. Within the Rotterdam Study, we followed COPD subjects until the first COPD exacerbation, or end of follow-up. Cardiovascular indication for β-blockers use was defined as a history of hypertension, coronary heart disease, atrial fibrillation and/or heart failure at baseline. The association between β-blockers use and COPD exacerbations was assessed using Cox proportional hazards models adjusted for age, sex, smoking, incident cardiovascular disease (i.e. heart failure, hypertension, atrial fibrillation and/or coronary heart disease during follow-up), respiratory drugs and nitrates. In total, 1312 COPD patients with a mean age of 69.7±9.2 years were included. In patients with a cardiovascular indication (n=755, mean age of 70.4±8.8 years), current use of cardioselective β-blockers was significantly associated with a reduced risk of COPD exacerbations (HR 0.69, 95% CI 0.57-0.85). In contrast, in subjects without a cardiovascular indication (n=557, mean age of 68.8±9.7 years), current use of cardioselective β-blockers was not associated with an altered risk of COPD exacerbations (HR 0.94, 95% CI 0.55-1.62). Use of cardioselective β-blockers reduced the risk of exacerbations in COPD patients with concomitant cardiovascular disease. Therefore, the potential benefits of β-blockers might be confined to COPD patients with cardiovascular disease.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: L. Karimi has nothing to disclose. Conflict of interest: L. Lahousse reports grants from AstraZeneca and Chiesi (both awards), and expert consultation for Boehringer Ingelheim GmbH and Novartis, outside the submitted work. Conflict of interest: P. De Nocker has nothing to disclose. Conflict of interest: B.H. Stricker has nothing to disclose. Conflict of interest: G.G. Brusselle reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis, GlaxoSmithKline, Sanofi and Teva, outside the submitted work. Conflict of interest: K.M.C. Verhamme works for a research group that, in the past, has received unconditional research grants from Pfizer, Boehringer Ingelheim, Yamanouchi and GSK, none of which is related to the content of this paper.
Figures
References
-
- Singh D, Agusti A, Anzueto A, et al. . Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: The GOLD science committee report 2019. Eur Respir J 2019; 53: 1900164. - PubMed
-
- GOLD. Global Strategy for Diagnosis and Prevention of COPD. 2020. https://goldcopd.org/gold-reports/ Date last accessed: August 1, 2020.
-
- Anees Ur R, Ahmad Hassali MA, Muhammad SA, et al. . The economic burden of chronic obstructive pulmonary disease (COPD) in the USA, Europe, and Asia: Results from a systematic review of the literature. Expert Rev Pharmacoeconom Outcomes Res 2020; 20: 661–672. - PubMed
-
- Chen W, Thomas J, Sadatsafavi M, et al. . Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Lancet Respir Med 2015; 3: 631–639. - PubMed
LinkOut - more resources
Full Text Sources