

Left ventricular function, strain, and infarct characteristics in patients with transient ST-segment elevation myocardial infarction compared to ST-segment and non-ST-segment elevation myocardial infarctions
- PMID: 34195800
- PMCID: PMC9159742
- DOI: 10.1093/ehjci/jeab114
Left ventricular function, strain, and infarct characteristics in patients with transient ST-segment elevation myocardial infarction compared to ST-segment and non-ST-segment elevation myocardial infarctions
Abstract
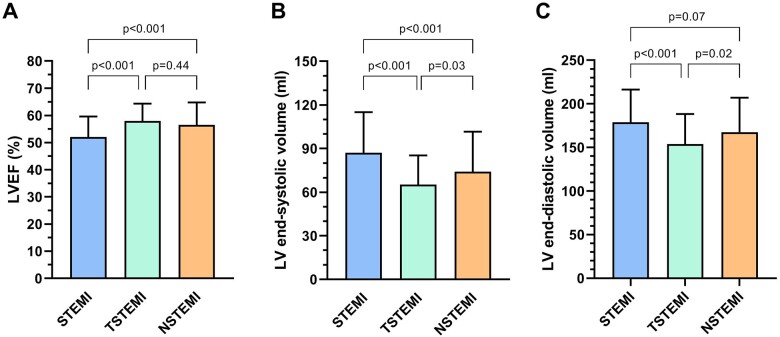
Aims: This study aims to explore cardiovascular magnetic resonance (CMR)-derived left ventricular (LV) function, strain, and infarct size characteristics in patients with transient ST-segment elevation myocardial infarction (TSTEMI) compared to patients with ST-segment and non-ST-segment elevation myocardial infarctions (STEMI and NSTEMI, respectively).
Methods and results: In total, 407 patients were enrolled in this multicentre observational prospective cohort study. All patients underwent CMR examination 2-8 days after the index event. CMR cine imaging was performed for functional assessment and late gadolinium enhancement to determine infarct size and identify microvascular obstruction (MVO). TSTEMI patients demonstrated the highest LV ejection fraction and the most preserved global LV strain (longitudinal, circumferential, and radial) across the three groups (overall P ≤ 0.001). The CMR-defined infarction was less frequently observed in TSTEMI than in STEMI patients [77 (65%) vs. 124 (98%), P < 0.001] but was comparable with NSTEMI patients [77 (65%) vs. 66 (70%), P = 0.44]. A remarkably smaller infarct size was seen in TSTEMI compared to STEMI patients [1.4 g (0.0-3.9) vs. 13.5 g (5.3-26.8), P < 0.001], whereas infarct size was not significantly different from that in NSTEMI patients [1.4 g (0.0-3.9) vs. 2.1 g (0.0-8.6), P = 0.06]. Whilst the presence of MVO was less frequent in TSTEMI compared to STEMI patients [5 (4%) vs. 53 (31%), P < 0.001], no significant difference was seen compared to NSTEMI patients [5 (4%) vs. 5 (5%), P = 0.72].
Conclusion: TSTEMI yielded favourable cardiac LV function, strain, and infarct-related scar mass compared to STEMI and NSTEMI. LV function and infarct characteristics of TSTEMI tend to be more similar to NSTEMI than STEMI.
Keywords: cardiovascular magnetic resonance imaging; infarct size; myocardial tissue characteristics; strain; transient ST-segment elevation myocardial infarction.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures



References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DAet al. ; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol 2018;72:2231–64. - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno Het al. ; ESC Scientific Document Group . 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119–77. - PubMed
-
- Collet JP, Thiele H, Barbato E, Barthelemy O, Bauersachs J, Bhatt DLet al. . 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2021;42:1289–367. - PubMed
-
- Badings EA, Remkes WS, The SH, Dambrink JE, Tjeerdsma G, Rasoul Set al. . Early or late intervention in patients with transient ST-segment elevation acute coronary syndrome: subgroup analysis of the ELISA-3 trial. Catheter Cardiovasc Interv 2016;88:755–64. - PubMed
-
- Terkelsen CJ, Norgaard BL, Lassen JF, Poulsen SH, Gerdes JC, Sloth Eet al. . Potential significance of spontaneous and interventional ST-changes in patients transferred for primary percutaneous coronary intervention: observations from the ST-MONitoring in Acute Myocardial Infarction study (The MONAMI study). Eur Heart J 2006;27:267–75. - PubMed
