

Systematic Review of PD-1/PD-L1 Inhibitors in Oncology: From Personalized Medicine to Public Health
- PMID: 34196068
- PMCID: PMC8488782
- DOI: 10.1002/onco.13887
Systematic Review of PD-1/PD-L1 Inhibitors in Oncology: From Personalized Medicine to Public Health
Abstract
Background: To review and summarize all U.S. Food and Drug Administration (FDA) approvals of programmed death (PD)-1 and PD-ligand 1 blocking antibodies (collectively referred to as PD-[L]1 inhibitors) over a 6-year period and corresponding companion/complementary diagnostic assays.
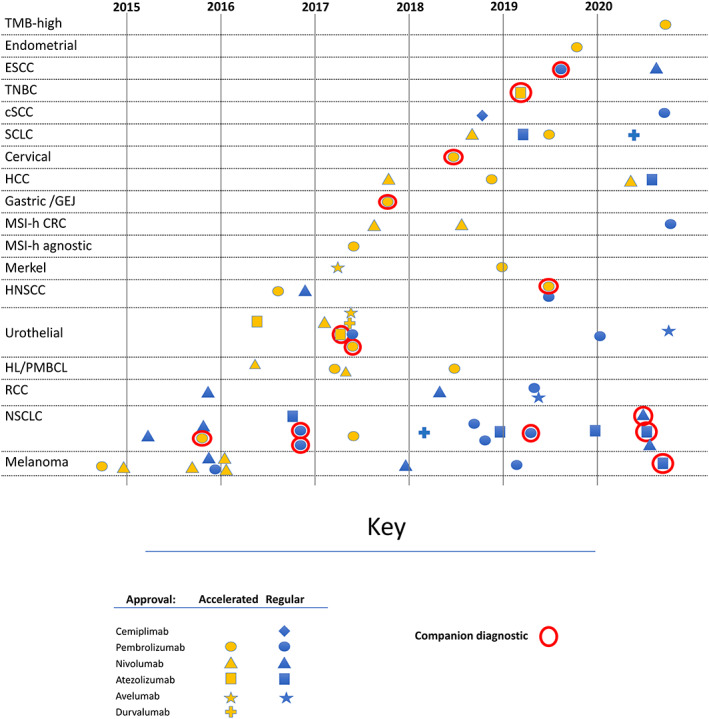
Materials and methods: To determine the indications and pivotal trials eligible for inclusion, approval letters and package inserts available on Drugs@FDA were evaluated for approved PD-[L]1 inhibitors to identify all new indications granted from the first approval of a PD-[L]1 inhibitor on September 4, 2014, through September 3, 2020. The corresponding FDA drug and device reviews from the marketing applications for the approved indications were identified through FDA internal records. Two reviewers independently extracted information for the endpoints, efficacy data, basis for approval, type of regulatory approval, and corresponding in vitro diagnostic device test. The results were organized by organ system and tumor type.
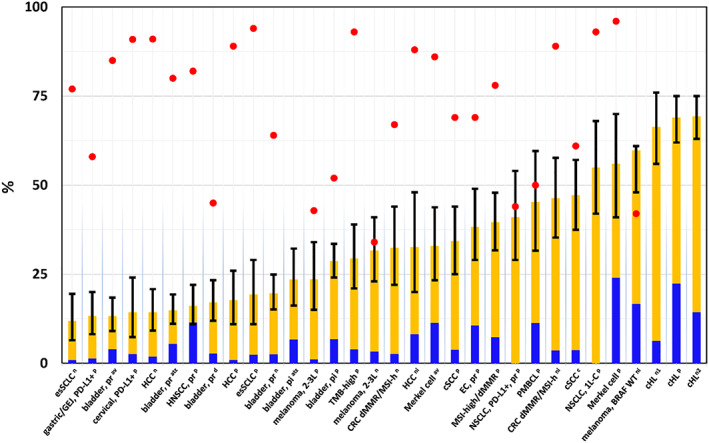
Results: Of 70 Biologic Licensing Application or supplement approvals that resulted in new indications, 32 (46%) were granted based on response rate (ORR) and durability of response, 26 (37%) on overall survival, 9 (13%) on progression-free survival, 2 (3%) on recurrence-free survival, and 1 (1%) on complete response rate. Most ORR-based approvals were granted under the accelerated approval provisions and were supported with prolonged duration of response. Overall, 21% of approvals were granted with a companion diagnostic. Efficacy results according to tumor type are discussed.
Conclusion: PD-[L]1 inhibitors are an effective anticancer therapy in a subset of patients. This class of drugs has provided new treatment options for patients with unmet need across a wide variety of cancer types. Yet, the modest response rates in several tumor types signal a lack of understanding of the biology of these diseases. Further preclinical and clinical investigation may be required to identify a more appropriate patient population, particularly as drug development continues and additional treatment alternatives become available.
Implications for practice: The number of PD-[L]1 inhibitors in drug development and the associated companion and complementary diagnostics have led to regulatory challenges and questions regarding generalizability of trial results. The interchangeability of PD-L1 immunohistochemical assays between PD-1/PD-L1 drugs is unclear. Furthermore, robust responses in some patients with low levels of PD-L1 expression have limited the use of PD-L1 as a predictive biomarker across all cancers, particularly in the setting of diseases with few alternative treatment options. This review summarizes the biomarker thresholds and assays approved as complementary and companion diagnostics and provides regulatory perspective on the role of biomarkers in oncology drug development.
Keywords: Checkpoint inhibitor; Companion diagnostic; Food and Drug Administration; Regulatory science.
Published 2021. This article is a U.S. Government work and is in the public domain in the USA. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- In vitro companion diagnostic devices : Guidance for Industry and Food and Drug Administration Staff. U.S. Food and Drug Administration. 2014. Available at https://www.fda.gov/media/81309/download. Accessed March 17, 2021.
-
- Accelerated approval program . 2020. U.S. Food and Drug Administration. Available at https://www.fda.gov/drugs/information-healthcare-professionals-drugs/acc.... Accessed March 17, 2021.
-
- Shamseer L, Moher D, Clarke M et al. Preferred reporting items for systematic review and meta‐analysis protocols (PRISMA‐P) 2015: Elaboration and explanation. BMJ 2015;349:g7647. - PubMed
-
- Robert C, Ribas A, Wolchok JD et al. Anti‐programmed‐death‐receptor‐1 treatment with pembrolizumab in ipilimumab‐refractory advanced melanoma: A randomised dose‐comparison cohort of a phase 1 trial. Lancet 2014;384:1109–1117. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
