

Antipsychotic Polypharmacy for the Management of Schizophrenia: Evidence and Recommendations
- PMID: 34196945
- PMCID: PMC8318953
- DOI: 10.1007/s40265-021-01556-4
Antipsychotic Polypharmacy for the Management of Schizophrenia: Evidence and Recommendations
Abstract
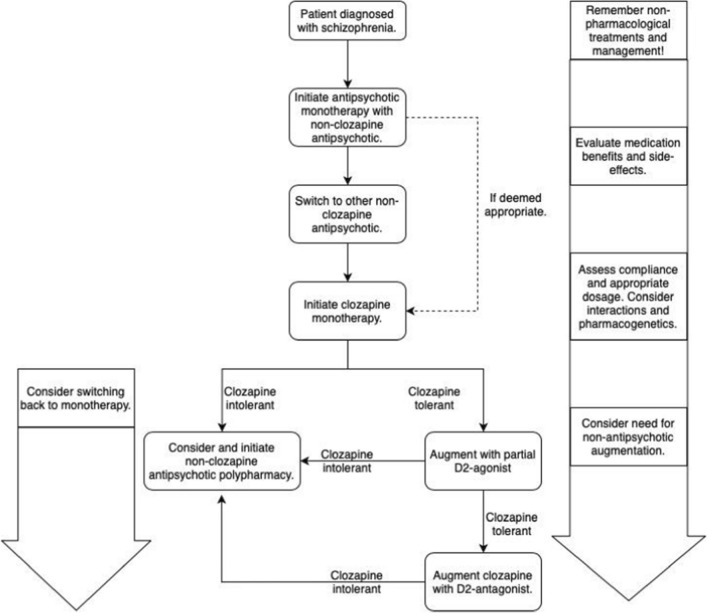
Schizophrenia is a debilitating illness with a lifetime prevalence estimate of 0.6% and consists of symptoms from the positive, negative, and cognitive domains. Social support, therapy, psychoeducation, and overall case management are very important aspects of the treatment of schizophrenia. However, as abnormalities in neurotransmission are one of the key findings of schizophrenia pathology, pharmacotherapies are cornerstones of the management of schizophrenia. Antipsychotics have been used as the primary pharmacological treatment of schizophrenia. These agents often have a good effect on reducing positive symptoms, but may not markedly improve negative symptoms or cognitive defects. However, at least 20% of individuals with schizophrenia do not experience a substantial response from monotherapy with antipsychotics. Further, despite evolving treatment protocols and advances in early recognition of the disorder, 70% of patients with schizophrenia require long-term, even lifetime, medication to control their symptoms and do not achieve complete recovery. To address these shortcomings, clinicians and research scientists have explored different combinations of treatments, polypharmacy, to improve the treatment of patients. Antipsychotic polypharmacy has been shown to cause more side effects than monotherapy, which is the main reason why most treatment guidelines caution against it. Antipsychotic monotherapy should be strived for and clozapine should be tried at the latest if two monotherapy trials with other antipsychotics have failed and no absolute contraindications exist. If residual symptoms exist despite trials of adequate dose and duration, other reasons that may reduce treatment effect should be ruled out. Long-acting injectables or blood concentration measurements should be considered to affirm compliance and proper serum levels. Antipsychotic polypharmacy should be considered and discussed with patients from whom the aforementioned procedures do not produce a satisfactory treatment result. In some cases, antipsychotic polypharmacy may produce better results than other forms of treatment augmentation, such as benzodiazepines. In particular, combining aripiprazole with clozapine may be effective in reducing treatment side effects or residual symptoms, and this is likely to hold true for combining other partial dopamine D2 agonists with clozapine as well, although currently scant data exist. More research is needed, both in controlled but also real-world settings, to define optimal antipsychotic polypharmacy and/or other psychotropic treatment augmentation strategies for specific patient groups and situations.
© 2021. The Author(s).
Conflict of interest statement
Jari Tiihonen reports personal fees from the Finnish Medicines Agency (Fimea), European Medicines Agency, Eli Lilly, Janssen-Cilag, Lundbeck, and Otsuka; is a member of an advisory board for Lundbeck; has participated in research projects funded by grants from Janssen-Cilag and Eli Lilly to his employing institution, and has received grants from the Stanley Foundation and Sigrid Jusélius Foundation. Markku Lähteenvuo is a board member of Genomi Solutions Ltd. and Nursie Health Ltd., and has received honoraria from Sunovion Ltd., Orion Pharma Ltd. Otsuka Ltd., Lundbeck Ltd., and Janssen-Cilag.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
