

Risk for Acquiring Coronavirus Disease Illness among Emergency Medical Service Personnel Exposed to Aerosol-Generating Procedures
- PMID: 34197282
- PMCID: PMC8386780
- DOI: 10.3201/eid2709.210363
Risk for Acquiring Coronavirus Disease Illness among Emergency Medical Service Personnel Exposed to Aerosol-Generating Procedures
Abstract
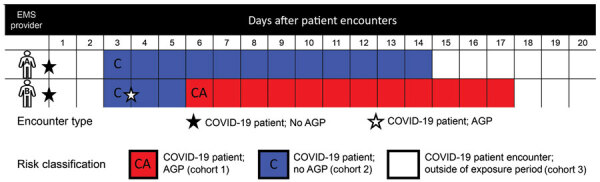
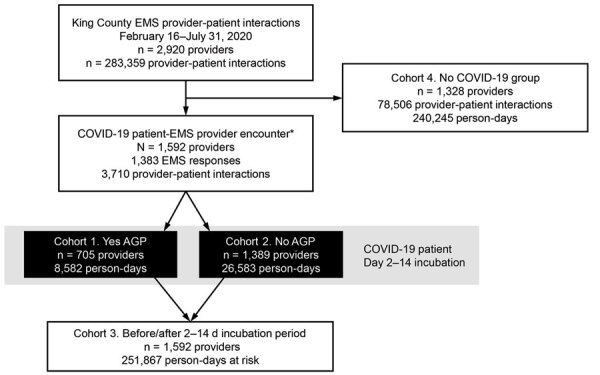
We investigated the risk of coronavirus disease (COVID-19)- patients transmitting severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) to emergency medical service (EMS) providers, stratified by aerosol-generating procedures (AGP), in King County, Washington, USA, during February 16-July 31, 2020. We conducted a retrospective cohort investigation using a statewide COVID-19 registry and identified 1,115 encounters, 182 with ≥1 AGP. Overall, COVID-19 incidence among EMS personnel was 0.57 infections/10,000 person-days. Incidence per 10,000 person-days did not differ whether or not infection was attributed to a COVID-19 patient encounter (0.28 vs. 0.59; p>0.05). The 1 case attributed to a COVID-19 patient encounter occurred within an at-risk period and involved an AGP. We observed a very low risk for COVID-19 infection attributable to patient encounters among EMS first responders, supporting clinical strategies that maintain established practices for treating patients in emergency conditions.
Keywords: COVID-19; SARS-COV-2; aerosol transmission; aerosol-generating procedures; cardiac arrest; coronavirus disease; emergency medical services; emergency treatment; health occupations; medical first responders; public health; public health readiness; respiratory infections; severe acute respiratory syndrome coronavirus 2; viruses; zoonoses.
Figures
References
-
- McMichael TM, Currie DW, Clark S, Pogosjans S, Kay M, Schwartz NG, et al.; Public Health–Seattle and King County, EvergreenHealth, and CDC COVID-19 Investigation Team. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. N Engl J Med. 2020;382:2005–11. 10.1056/NEJMoa2005412 - DOI - PMC - PubMed
-
- Yang BY, Barnard LM, Emert JM, Drucker C, Schwarcz L, Counts CR, et al. Clinical characteristics of patients with coronavirus disease 2019 (COVID-19) receiving emergency medical services in King County, Washington. JAMA Netw Open. 2020;3:e2014549. 10.1001/jamanetworkopen.2020.14549 - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention (CDC). Cluster of severe acute respiratory syndrome cases among protected health-care workers—Toronto, Canada, April 2003. MMWR Morb Mortal Wkly Rep. 2003;52:433–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
