

Inequalities of visceral leishmaniasis case-fatality in Brazil: A multilevel modeling considering space, time, individual and contextual factors
- PMID: 34197454
- PMCID: PMC8279375
- DOI: 10.1371/journal.pntd.0009567
Inequalities of visceral leishmaniasis case-fatality in Brazil: A multilevel modeling considering space, time, individual and contextual factors
Abstract
Background: In Brazil, case-fatality from visceral leishmaniasis (VL) is high and characterized by wide differences between the various political-economic units, the federated units (FUs). This study was designed to investigate the association between factors at the both FU and individual levels with the risk of dying from VL, after analysing the temporal trend and the spatial dependency for VL case-fatality.
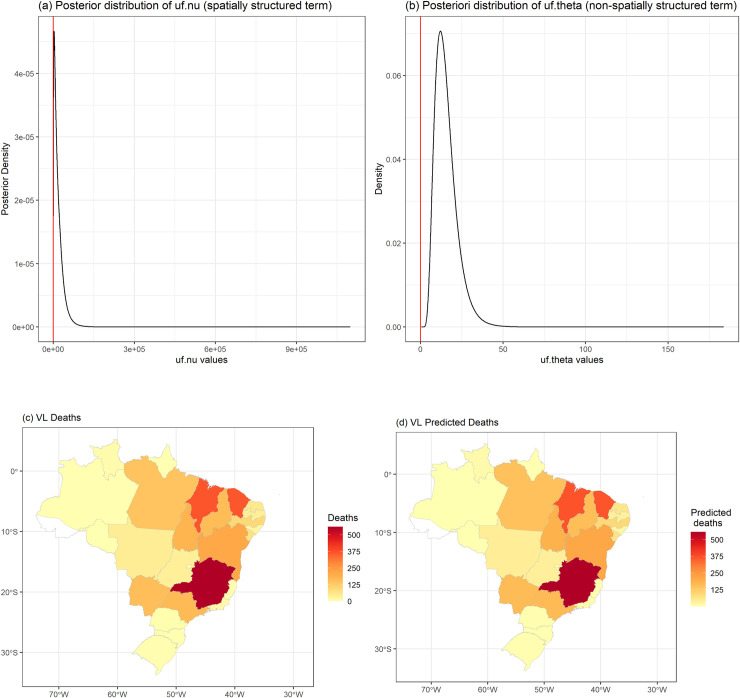
Methodology: The analysis was based on individual and aggregated data of the Reportable Disease Information System-SINAN (Brazilian Ministry of Health). The temporal and spatial distributions of the VL case-fatality between 2007 and 2017 (27 FUs as unit of analysis) were considered together with the individual characteristics and many other variables at the FU level (socioeconomic, demographic, access to health and epidemiological indicators) in a mixed effects models or multilevel modeling, assuming a binomial outcome distribution (death from VL).
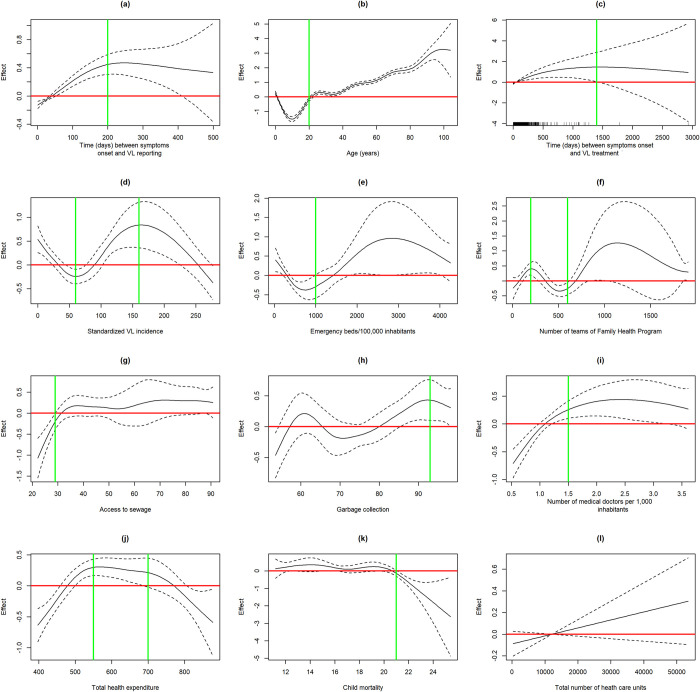
Findings: A linear increasing temporal tendency (4%/year) for VL case-fatality was observed between 2007 and 2017. There was no similarity between the case-fatality rates of neighboring FUs (non-significant spatial term), although these rates were heterogeneous in this spatial scale of analysis. In addition to the known individual risk factors age, female gender, disease's severity, bacterial co-infection and disease duration, low level schooling and unavailability of emergency beds and health professionals (the last two only in univariate analysis) were identified as possibly related to VL death risk. Lower VL incidence was also associated to VL case-fatality, suggesting that unfamiliarity with the disease may delay appropriate medical management: VL patients with fatal outcome were notified and had VL treatment started 6 and 3 days later, respectively, in relation to VL cured patients. Access to garbage collection, marker of social and economic development, seems to be protective against the risk of dying from VL. Part of the observed VL case-fatality variability in Brazil could not be explained by the studied variables, suggesting that factors linked to the intra FU environment may be involved.
Conclusions: This study aimed to identify epidemiological conditions and others related to access to the health system possibly linked to VL case-fatality, pointing out new prognostic determinants subject to intervention.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- World Health Organization (WHO). Epidemiology of Leishmaniasis. Available from: http://www.who.int/leishmaniasis/burden/en/. Accessed on October 1, 2020.
-
- World Health Organization (WHO). Weekly epidemiological record. No 22, 91, 285–296. Available at https://apps.who.int/iris/handle/10665/254451.
-
- World Health Organization (WHO). Kala-Azar elimination programme: report of a WHO consultation of partners, Geneva, Switzerland, 2015. Feb 10–11. Available at: https://apps.who.int/iris/handle/10665/185042.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
