

Over 100 Years of Rift Valley Fever: A Patchwork of Data on Pathogen Spread and Spillover
- PMID: 34198898
- PMCID: PMC8227530
- DOI: 10.3390/pathogens10060708
Over 100 Years of Rift Valley Fever: A Patchwork of Data on Pathogen Spread and Spillover
Abstract
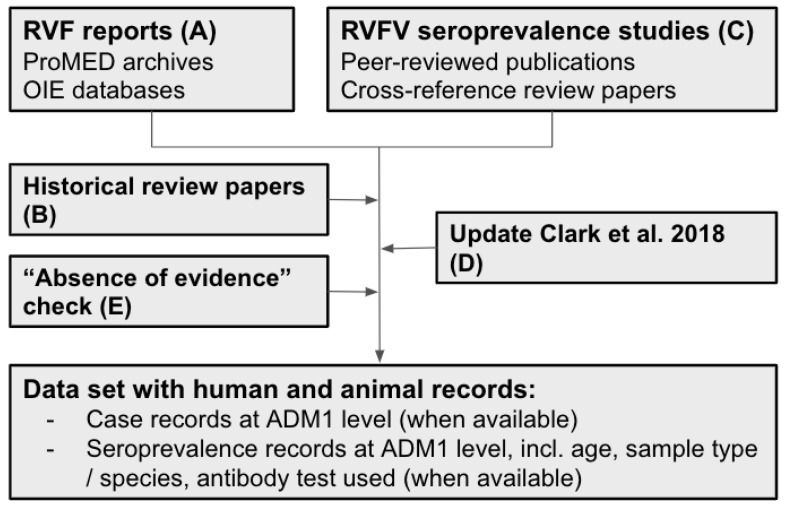
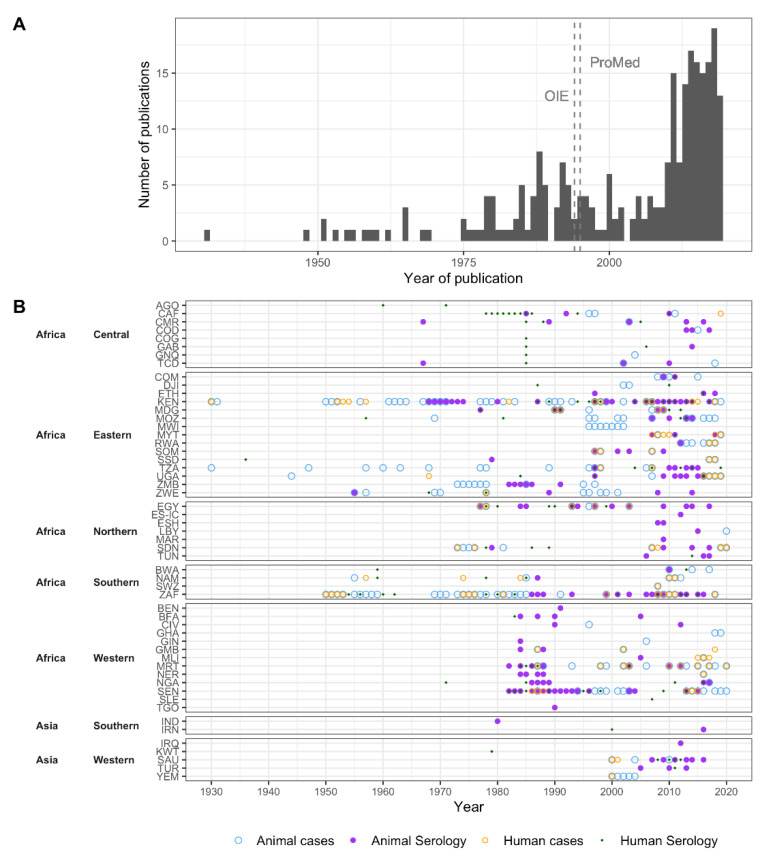
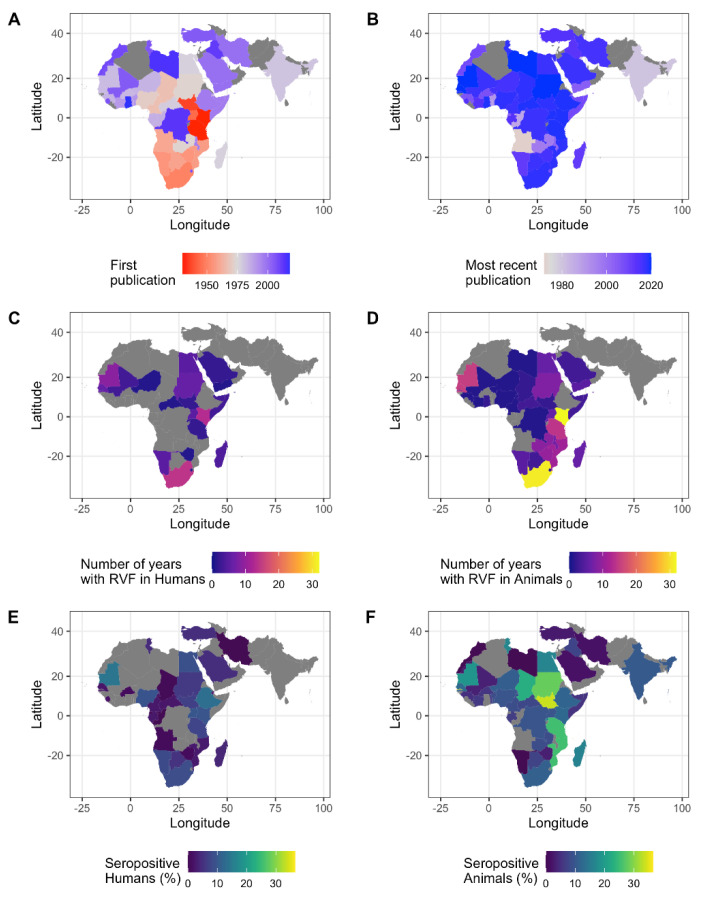
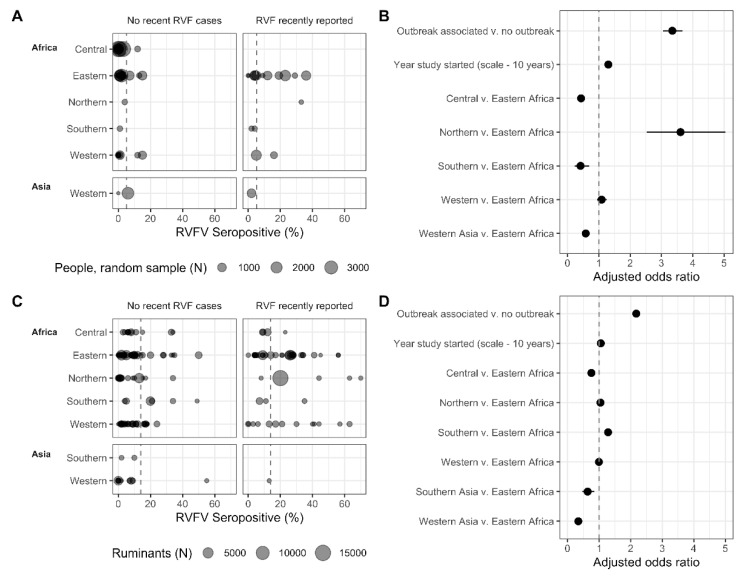
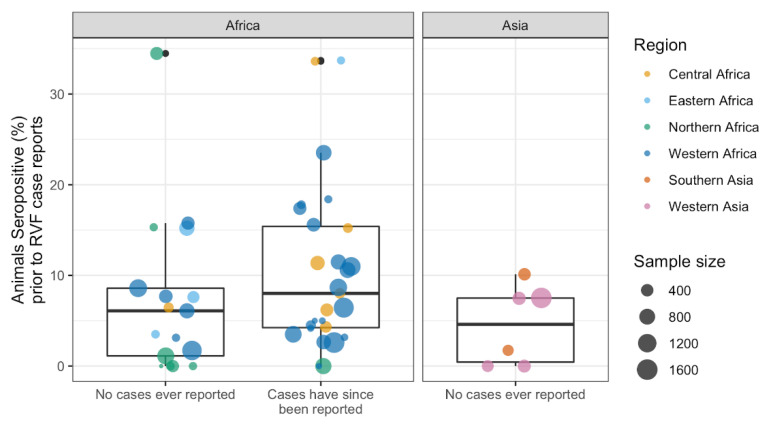
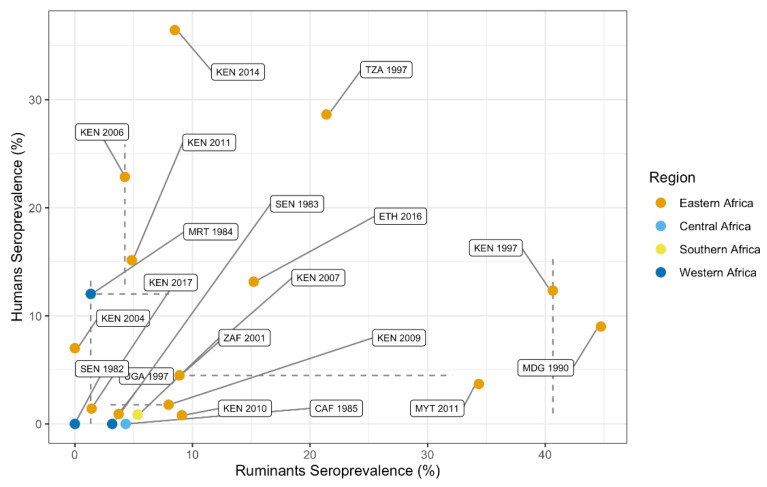
During the past 100 years, Rift Valley fever virus (RVFV), a mosquito-borne virus, has caused potentially lethal disease in livestock, and has been associated with significant economic losses and trade bans. Spillover to humans occurs and can be fatal. Here, we combined data on RVF disease in humans (22 countries) and animals (37 countries) from 1931 to 2020 with seroprevalence studies from 1950 to 2020 (n = 228) from publicly available databases and publications to draw a more complete picture of the past and current RVFV epidemiology. RVFV has spread from its original locus in Kenya throughout Africa and into the Arabian Peninsula. Throughout the study period seroprevalence increased in both humans and animals, suggesting potentially increased RVFV exposure. In 24 countries, animals or humans tested positive for RVFV antibodies even though outbreaks had never been reported there, suggesting RVFV transmission may well go unnoticed. Among ruminants, sheep were the most likely to be exposed during RVF outbreaks, but not during periods of cryptic spread. We discuss critical data gaps and highlight the need for detailed study descriptions, and long-term studies using a one health approach to further convert the patchwork of data to the tale of RFV epidemiology.
Keywords: ProMED; Rift Valley fever phlebovirus; bunyavirales; mosquito-borne disease; notifiable disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Harcourt M.P., Bowring C.C. Annual Report on the East Africa Protectorate for 1912–1913. Barclay and Fry; Southwark, UK: 1914. p. 27.
-
- Daubney R., Hudson J.R., Garnham P.C. Enzootic Hepatitis or Rift Valley Fever. An Undescribed Virus Disease of Sheep Cattle and Man from East Africa. J. Pathol. Bacteriol. 1931;34:545–579. doi: 10.1002/path.1700340418. - DOI
-
- ICTV Taxonomy History: Rift Valley Fever Phlebovirus. [(accessed on 21 January 2021)]; Available online: https://talk.ictvonline.org/taxonomy/p/taxonomy-history?taxnode_id=20190....
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
