

Cardiac Amyloidosis with Discordant QRS Voltage between Frontal and Precordial Leads
- PMID: 34199044
- PMCID: PMC8306315
- DOI: 10.3390/medicina57070660
Cardiac Amyloidosis with Discordant QRS Voltage between Frontal and Precordial Leads
Abstract
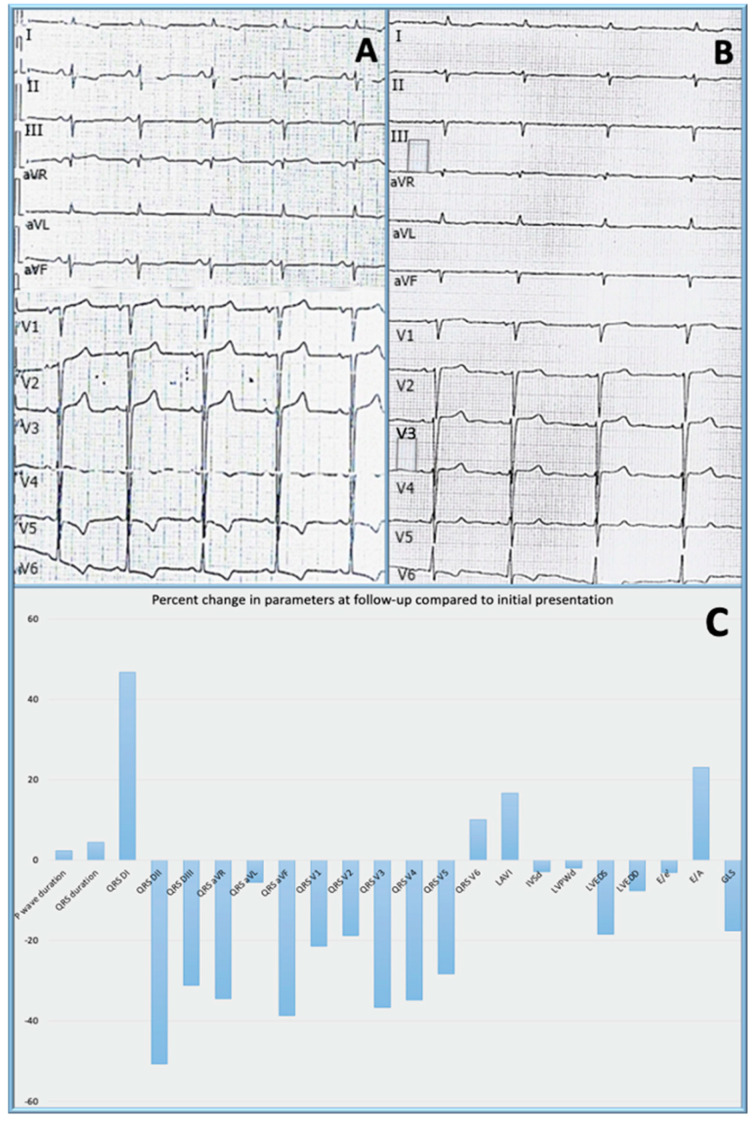
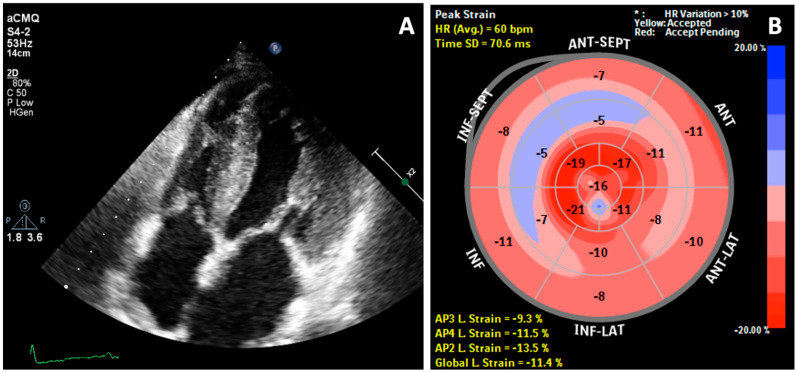
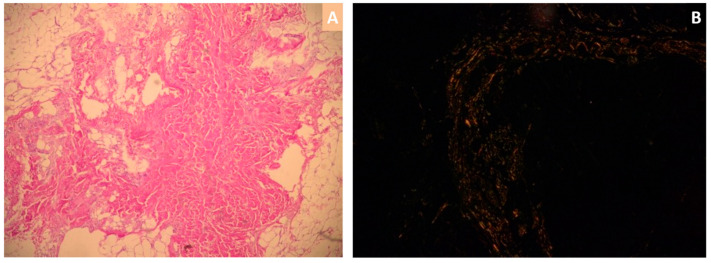
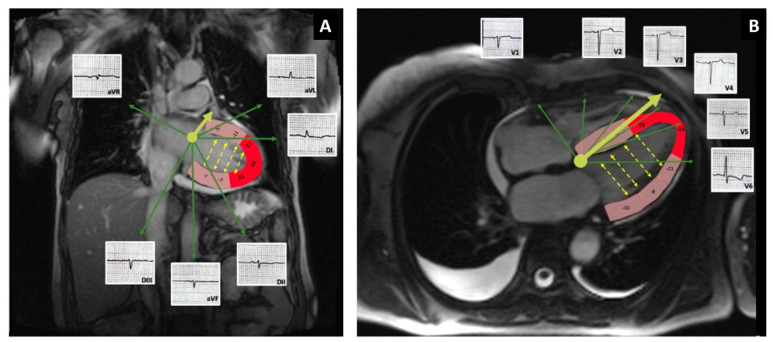
Among the different types, immunoglobulin light chain (AL) cardiac amyloidosis is associated with the highest morbidity and mortality. The outcome, however, is significantly better when an early diagnosis is made and treatment initiated promptly. We present a case of cardiac amyloidosis with left ventricular hypertrophy criteria on the electrocardiogram. After 9 months of follow-up, the patient developed low voltage in the limb leads, while still maintaining the Cornell criteria for left ventricular hypertrophy as well. The relative apical sparing by the disease process, as well as decreased cancellation of the opposing left ventricular walls could be responsible for this phenomenon. The discordance between the voltage in the frontal leads and precordial leads, when present in conjunction with other findings, may be helpful in raising the clinical suspicion of cardiac amyloidosis.
Keywords: amyloidosis; cardiomyopathy; low voltage.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hirata Y., Kusunose K., Miki H., Yamada H. Improvement of global longitudinal strain following high-dose chemotherapy and autologous peripheral blood stem cell transplantation in patients with amyloid light-chain cardiac amyloidosis: A case report. Eur. Heart J. Case Rep. 2019;3:1–6. doi: 10.1093/ehjcr/ytz225. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
