

Association of Frailty with Adverse Outcomes in Patients with Suspected COVID-19 Infection
- PMID: 34199572
- PMCID: PMC8199640
- DOI: 10.3390/jcm10112472
Association of Frailty with Adverse Outcomes in Patients with Suspected COVID-19 Infection
Abstract
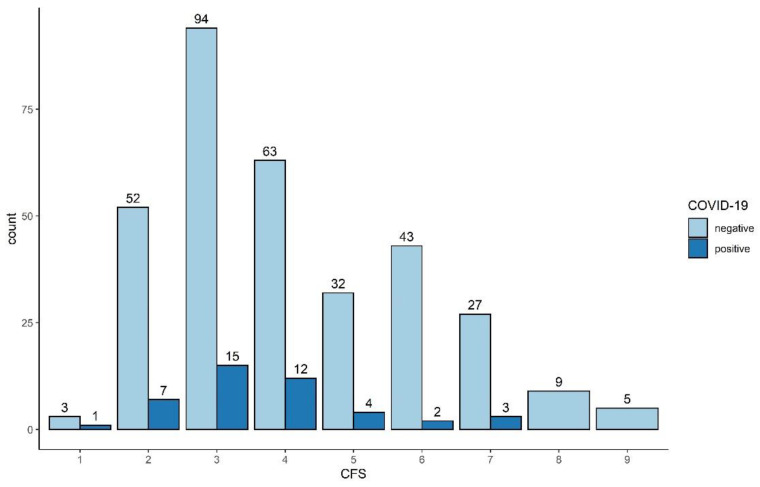
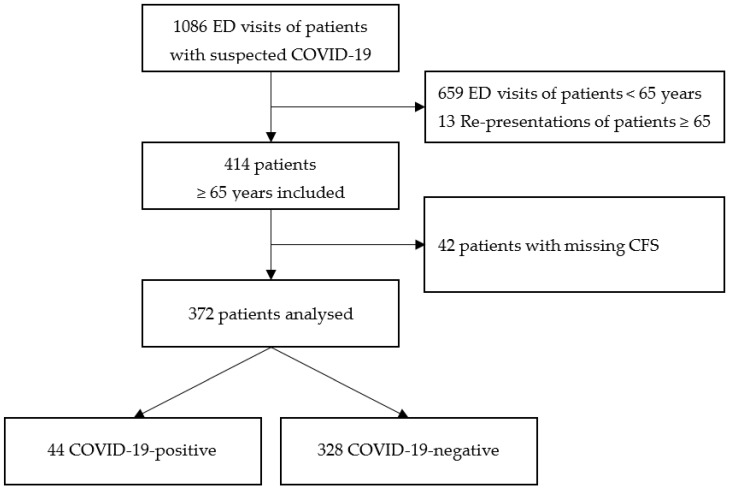
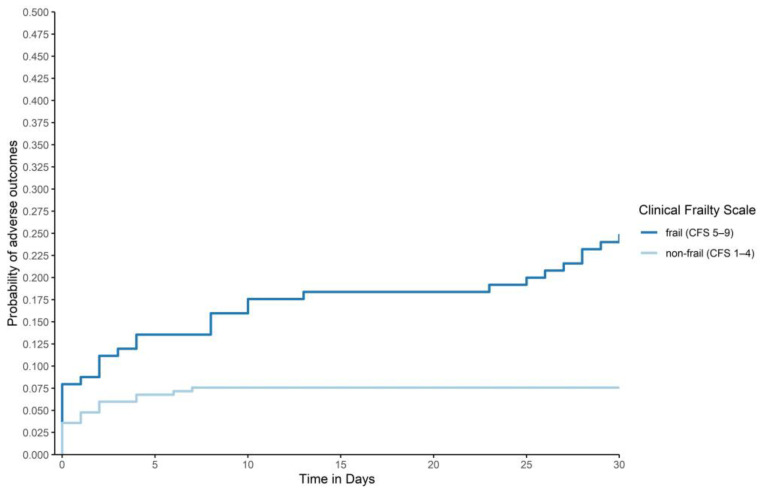
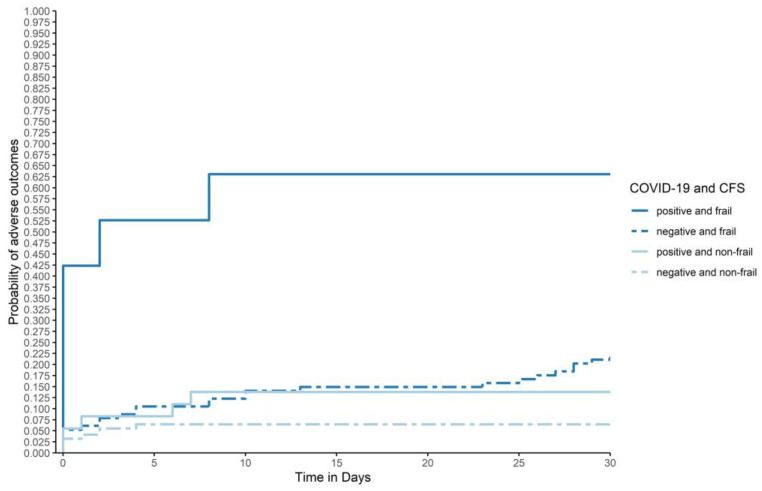
Older age and frailty are predictors of adverse outcomes in patients with COVID-19. In emergency medicine, patients do not present with the diagnosis, but with suspicion of COVID-19. The aim of this study was to assess the association of frailty and age with death or admission to intensive care in patients with suspected COVID-19. This single-centre prospective cohort study was performed in the Emergency Department of a tertiary care hospital. Patients, 65 years and older, with suspected COVID-19 presenting to the Emergency Department during the first wave of the pandemic were consecutively enrolled. All patients underwent nasopharyngeal SARS-CoV-2 PCR swab tests. Patients with a Clinical Frailty Scale (CFS) > 4, were considered to be frail. Associations between age, gender, frailty, and COVID-19 status with the composite adverse outcome of 30-day-intensive-care-admission and/or 30-day-mortality were tested. In the 372 patients analysed, the median age was 77 years, 154 (41.4%) were women, 44 (11.8%) were COVID-19-positive, and 125 (33.6%) were frail. The worst outcome was seen in frail COVID-19-patients with six (66.7%) adverse outcomes. Frailty (CFS > 4) and COVID-19-positivity were associated with an adverse outcome after adjustment for age and gender (frailty: OR 5.01, CI 2.56-10.17, p < 0.001; COVID-19: OR 3.47, CI 1.48-7.89, p = 0.003). Frailty was strongly associated with adverse outcomes and outperformed age as a predictor in emergency patients with suspected COVID-19.
Keywords: COVID-19; SARS-CoV-2; age; emergency department; frailty; intensive care; mortality.
Conflict of interest statement
Twerenbold reports research support from the Swiss National Science Foundation (Grant No P300PB_167803), the Swiss Heart Foundation, the Swiss Society of Cardiology, the Cardiovascular Research Foundation Basel, the University of Basel and the University Hospital Basel. None of the other authors have any conflicts of interest to declare.
Figures
References
-
- Chatterjee A., Wu G., Primakov S., Oberije C., Woodruff H., Kubben P., Henry R., Aries M.J., Beudel M., Noordzij P.G. Can predicting COVID-19 mortality in a European cohort using only demographic and comorbidity data surpass age-based prediction: An externally validated study. PLoS ONE. 2021;16:e0249920. doi: 10.1371/journal.pone.0249920. - DOI - PMC - PubMed
-
- Kim L., Garg S., O’Halloran A., Whitaker M., Pham H., Anderson E.J., Armistead I., Bennett N.M., Billing L., Como-Sabetti K. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-NET) Clin. Infect. Dis. 2020 doi: 10.1093/cid/ciaa1012. - DOI - PMC - PubMed
-
- Hewitt J., Carter B., Vilches-Moraga A., Quinn T.J., Braude P., Verduri A., Pearce L., Stechman M., Short R., Price A. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health. 2020;5:e444–e451. doi: 10.1016/S2468-2667(20)30146-8. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
