

May Bacterial Infections Trigger Bullous Pemphigoid? Case Report and Review of Literature
- PMID: 34200214
- PMCID: PMC8229970
- DOI: 10.3390/microorganisms9061235
May Bacterial Infections Trigger Bullous Pemphigoid? Case Report and Review of Literature
Abstract
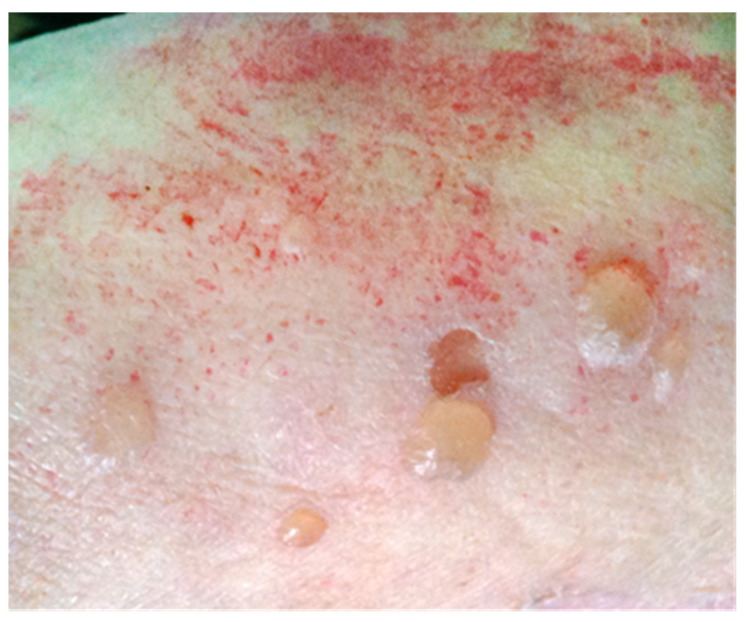
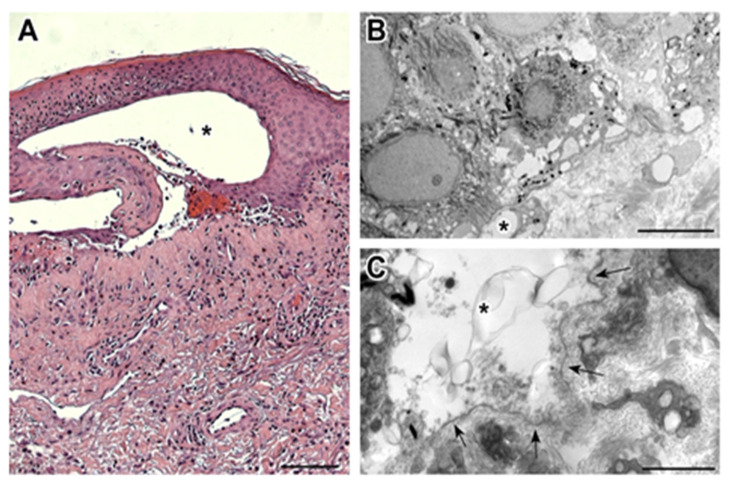
Bullous pemphigoid (BP) is an autoimmune blistering skin disease, mainly observed in the elderly. Infections have been suggested as possible disease triggers. However, infections may even heavily influence the disease clinical course and mortality. A 75-year-old woman was admitted to hospital for severe erythematosus blistering disease, accompanied by hyper-eosinophilia and hyper-IgE. The culture of bullous fluid was positive for Enterococcus faecalis, the blood culture was positive for Staphylococcus aureus, and the urine culture was positive for Proteus mirabilis and Escherichia coli. Moreover, circulating anti-BP180 IgG was present and the histopathological/ultrastructural examination of a lesional skin biopsy was compatible with BP. High eosinophil levels (up to 3170/µL) were found throughout the clinical course, while values below 1000/µL were associated with clinical improvement. The total IgE was 1273 IU/mL, and specific anti-G/V-penicillin/ampicillin IgE antibodies were positive. The patient had a complete clinical recovery in two months with methyl-prednisolone (40 then 20 mg/day) and low-dose azathioprine (50 mg/day) as a steroid-sparing agent. The steroid treatment was tapered until interruption during a one-year period and intravenous immunoglobulins have been administered for three years in order for azathioprine to also be interrupted. The patient stopped any treatment five years ago and, in this period, has always been in good health. In this case, the contemporaneous onset of different bacterial infections and BP is suggestive of bacterial infections acting as BP trigger(s), with allergic and autoimmune pathways contributing to the disease pathogenesis.
Keywords: IVIg; autoimmunity; bullous pemphigoid (BP); infections.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
