

Comparison of Extracapsular Stabilization Techniques Using an Ultrasonically Implanted Absorbable Bone Anchor (Weldix) after Cranial Cruciate Ligament Rupture in Cats-An In Vitro Study
- PMID: 34200227
- PMCID: PMC8227609
- DOI: 10.3390/ani11061695
Comparison of Extracapsular Stabilization Techniques Using an Ultrasonically Implanted Absorbable Bone Anchor (Weldix) after Cranial Cruciate Ligament Rupture in Cats-An In Vitro Study
Abstract
Background: This study evaluated joint stability after surgical repair of cranial cruciate ligament (CrCL)-deficient stifle joints in cats using a novel absorbable polylactide bone anchor in an ex vivo model.
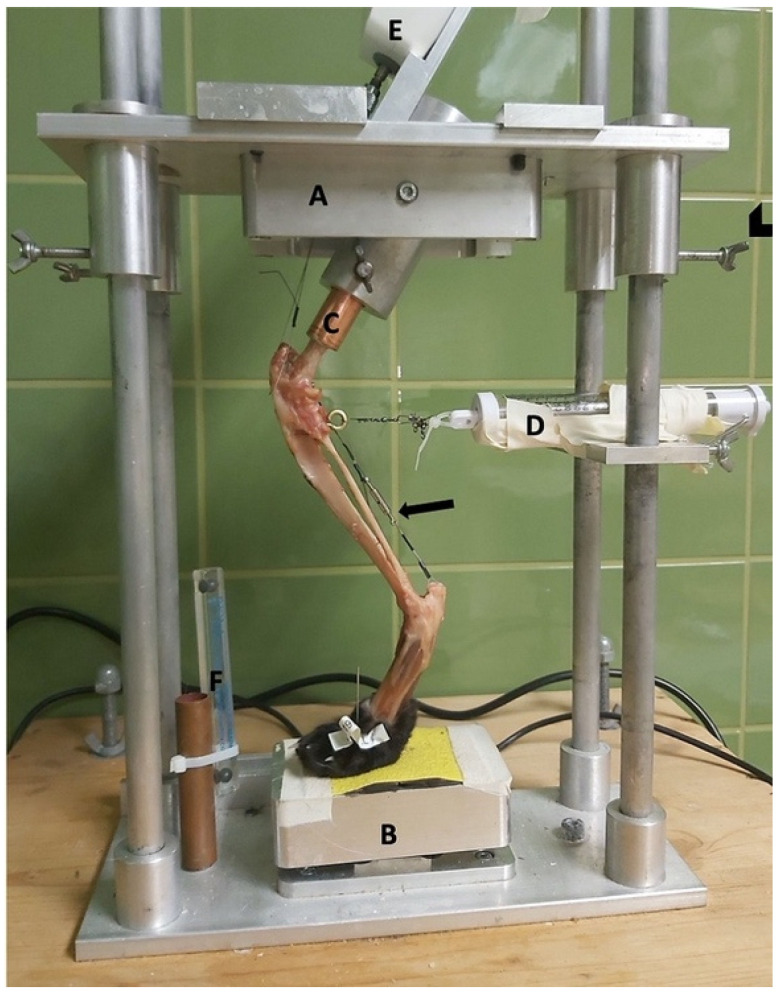
Methods: Thirty-six hindlimbs from cats with intact (Gi group) and transected CrCLs were treated with fabellotibial suture alone (GFW group), suture combined with an absorbable polylactide bone anchor (GWD group), or suture combined with a nonabsorbable bone anchor (GFT group), positioned in a limb press with predefined joint angles (stifle joint: 120 ± 5°; hock joint: 120 ± 5°) and loaded with 10%, 20%, and 30% of body mass (BM). Predefined points were measured on lateral radiographs and with a coordinate measurement machine. Distances on radiographs (mm) were measured and angles (°) were calculated to represent the craniocaudal movement and the internal rotation of the tibia.
Results: There were no differences for craniocaudal movement between Gi and GFW or GFT, but for GWD regarding angle measurement at 30% BM. For internal rotation, there was no significant difference between Gi and GFW or GWD, but for GFT.
Conclusion: The used absorbable polylactide bone-anchor was able to stabilize the stifle joint regarding internal rotation and craniocaudal movement as calculated from distance measurements.
Keywords: absorbable bone anchor; cat; cranial cruciate ligament rupture; fabellotibial suture.
Conflict of interest statement
Eva Schnabl-Feichter is a consultant for Arthrex GmbH, Munich, Germany. The company had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures




References
-
- Slocum B., Devine T. Cranial Tibial Wedge Osteotomy: A Technique for Eliminating Cranial Tibial Thrust in Cranial Cruciate Ligament Repair. J. Am. Vet. Med. Assoc. 1984;184:564–569. - PubMed
-
- Scavelli T.D., Schrader S.C. Nonsurgical Management of Rupture of the Cranial Cruciate Ligament in 18 Cats. J. Am. Anim. Hosp. Assoc. 1987;23:337–340.
LinkOut - more resources
Full Text Sources
Miscellaneous
