

Magnesium Metabolism in Chronic Alcohol-Use Disorder: Meta-Analysis and Systematic Review
- PMID: 34200366
- PMCID: PMC8229336
- DOI: 10.3390/nu13061959
Magnesium Metabolism in Chronic Alcohol-Use Disorder: Meta-Analysis and Systematic Review
Abstract
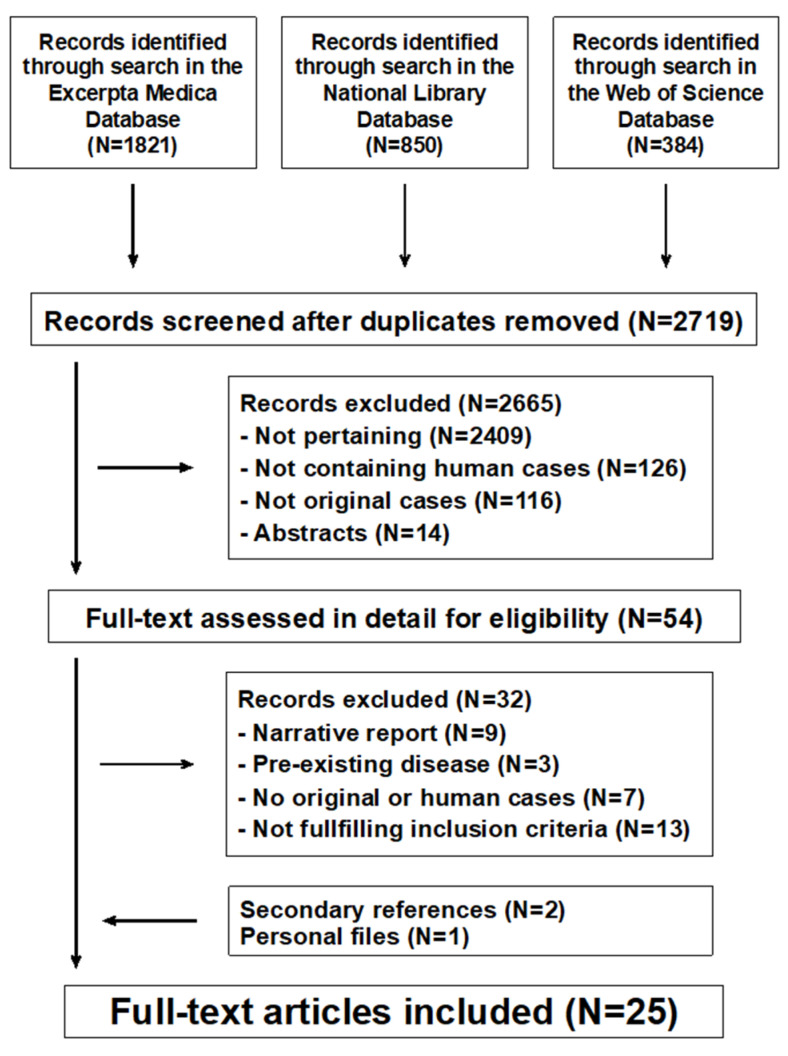
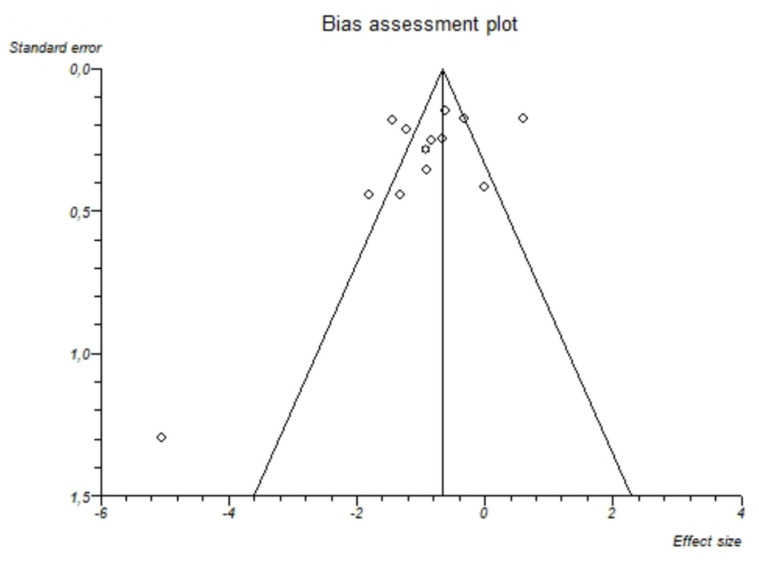
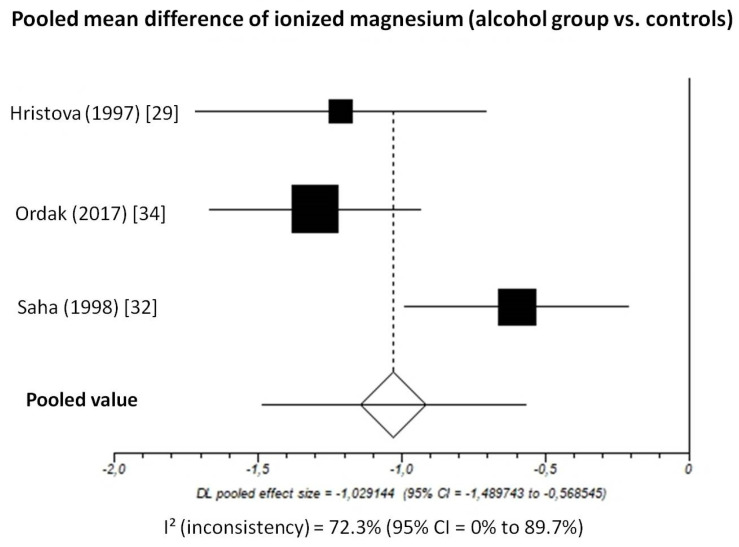
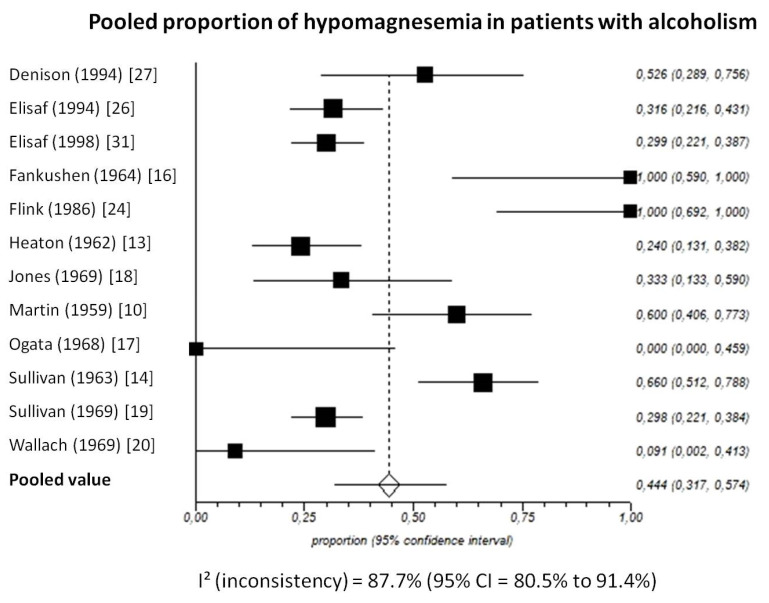
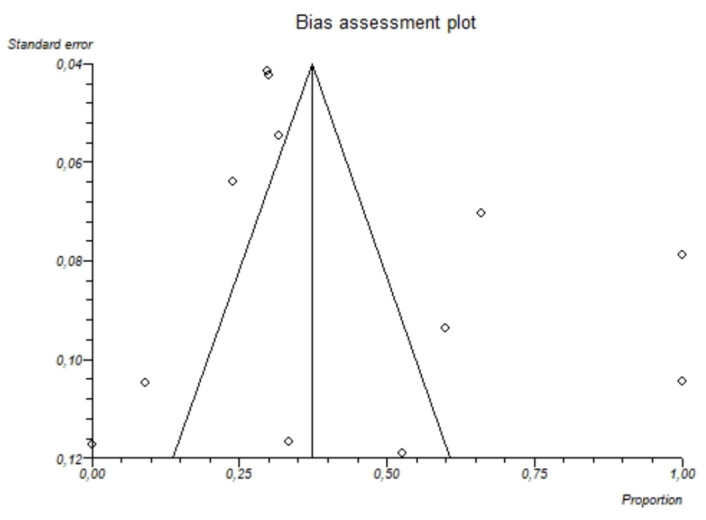
Chronic alcohol-use disorder has been imputed as a possible cause of dietary magnesium depletion. The purpose of this study was to assess the prevalence of hypomagnesemia in chronic alcohol-use disorder, and to provide information on intracellular magnesium and on its renal handling. We carried out a structured literature search up to November 2020, which returned 2719 potentially relevant records. After excluding non-significant records, 25 were retained for the final analysis. The meta-analysis disclosed that both total and ionized circulating magnesium are markedly reduced in chronic alcohol-use disorder. The funnel plot and the Egger's test did not disclose significant publication bias. The I2-test demonstrated significant statistical heterogeneity between studies. We also found that the skeletal muscle magnesium content is reduced and the kidney's normal response to hypomagnesemia is blunted. In conclusion, magnesium depletion is common in chronic alcohol-use disorder. Furthermore, the kidney plays a crucial role in the development of magnesium depletion.
Keywords: alcohol-use; depletion; diet; electrolytes; hypomagnesemia; kidney; magnesium.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Liberati A., Altman D.G., Tetzlaff J., Mulrow C., Gøtzsche P.C., Ioannidis J.P., Clarke M., Devereaux P.J., Kleijnen J., Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009;151:W65–W94. doi: 10.7326/0003-4819-151-4-200908180-00136. - DOI - PubMed
