

Hyperspectral Imaging (HSI)-A New Tool to Estimate the Perfusion of Upper Abdominal Organs during Pancreatoduodenectomy
- PMID: 34200412
- PMCID: PMC8201356
- DOI: 10.3390/cancers13112846
Hyperspectral Imaging (HSI)-A New Tool to Estimate the Perfusion of Upper Abdominal Organs during Pancreatoduodenectomy
Abstract
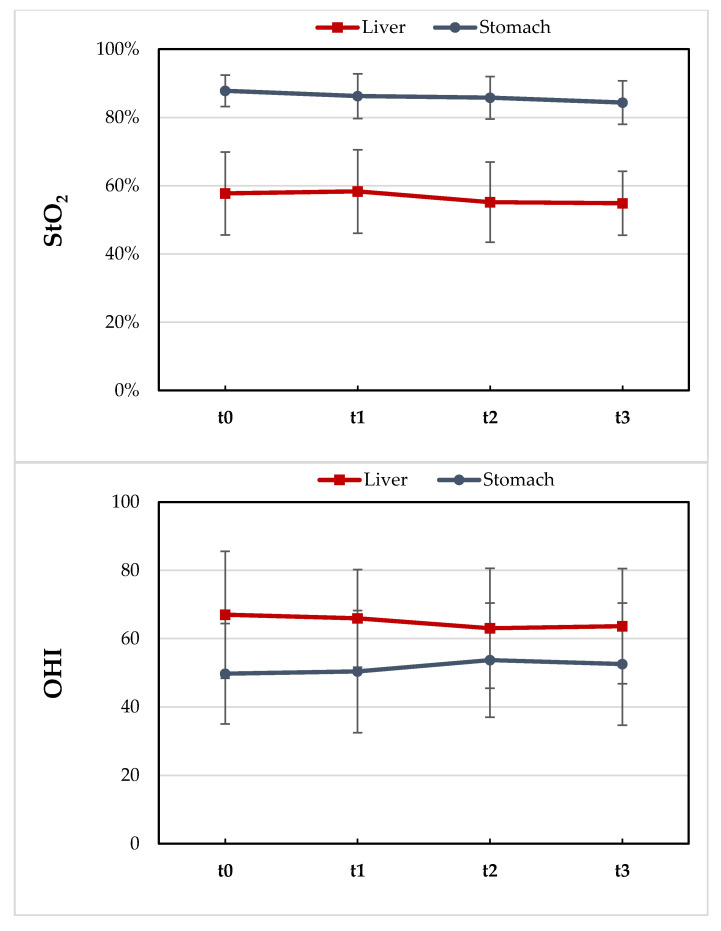
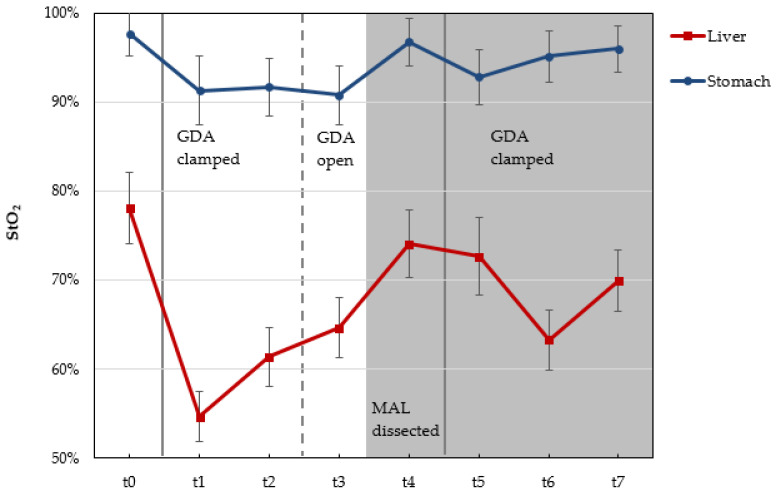
Hyperspectral imaging (HSI) in abdominal surgery is a new non-invasive tool for the assessment of the perfusion and oxygenation of various tissues and organs. Its benefit in pancreatic surgery is still unknown. The aim of this study was to evaluate the key impact of using HSI during pancreatoduodenectomy (PD). In total, 20 consecutive patients were included. HSI was recorded during surgery as part of a pilot study approved by the local Ethics Committee. Data were collected prospectively with the TIVITA® Tissue System. Intraoperative HS images were recorded before and after gastroduodenal artery (GDA) clamping. We detected four patients with celiac artery stenosis (CAS) caused by a median arcuate ligament (MAL). In two of these patients, a reduction in liver oxygenation (StO2) was discovered 15 and 30 min after GDA clamping. The MAL was divided in these patients. HSI showed an improvement of liver StO2 after MAL division (from 61% to 73%) in one of these two patients. There was no obvious decrease in liver StO2 in the other two patients with CAS. HSI, as a non-invasive procedure, could be helpful in evaluating liver and gastric perfusion during PD, which might assist surgeons in choosing the best surgical approach and in improving patients' outcomes.
Keywords: celiac artery stenosis (CAS); hyperspectral imaging (HSI); pancreatoduodenectomy (PD).
Conflict of interest statement
The authors declare no conflict of interest.
Figures







Similar articles
-
Intraoperative bowel perfusion quantification with hyperspectral imaging: a guidance tool for precision colorectal surgery.Surg Endosc. 2022 Nov;36(11):8520-8532. doi: 10.1007/s00464-022-09407-3. Epub 2022 Jul 14. Surg Endosc. 2022. PMID: 35836033
-
Hyperspectral imaging for perioperative monitoring of microcirculatory tissue oxygenation and tissue water content in pancreatic surgery - an observational clinical pilot study.Perioper Med (Lond). 2021 Dec 1;10(1):42. doi: 10.1186/s13741-021-00211-6. Perioper Med (Lond). 2021. PMID: 34847953 Free PMC article.
-
Intraoperative Assessment of Gastric Sleeve Oxygenation Using Hyperspectral Imaging in Esophageal Resection: A Feasibility Study.Visc Med. 2021 Jun;37(3):165-170. doi: 10.1159/000509304. Epub 2020 Aug 7. Visc Med. 2021. PMID: 34239918 Free PMC article.
-
Collaterals management during pancreatoduodenectomy in patients with celiac axis stenosis: A systematic review of the literature.Pancreatology. 2018 Jul;18(5):592-600. doi: 10.1016/j.pan.2018.05.003. Epub 2018 May 16. Pancreatology. 2018. PMID: 29776725 Review.
-
[Artificial intelligence and hyperspectral imaging for image-guided assistance in minimally invasive surgery].Chirurgie (Heidelb). 2022 Oct;93(10):940-947. doi: 10.1007/s00104-022-01677-w. Epub 2022 Jul 7. Chirurgie (Heidelb). 2022. PMID: 35798904 Review. German.
Cited by
-
The role of intraoperative hyperspectral imaging (HSI) in colon interposition after esophagectomy.BMC Surg. 2023 Mar 2;23(1):47. doi: 10.1186/s12893-023-01946-3. BMC Surg. 2023. PMID: 36864396 Free PMC article.
-
Hyperspectral Imaging as a Tool for Viability Assessment During Normothermic Machine Perfusion of Human Livers: A Proof of Concept Pilot Study.Transpl Int. 2022 May 16;35:10355. doi: 10.3389/ti.2022.10355. eCollection 2022. Transpl Int. 2022. PMID: 35651880 Free PMC article.
-
Clinical applications of hyperspectral imaging in gastroenterology and hepatology: A systematic review.Indian J Gastroenterol. 2025 Aug 6. doi: 10.1007/s12664-025-01836-x. Online ahead of print. Indian J Gastroenterol. 2025. PMID: 40768177 Review.
-
Hyperspectral imaging in living and deceased donor kidney transplantation.BMC Med Imaging. 2025 Jan 31;25(1):34. doi: 10.1186/s12880-025-01576-6. BMC Med Imaging. 2025. PMID: 39891083 Free PMC article.
-
Hyperspectral Imaging and Machine Perfusion in Solid Organ Transplantation: Clinical Potentials of Combining Two Novel Technologies.J Clin Med. 2021 Aug 27;10(17):3838. doi: 10.3390/jcm10173838. J Clin Med. 2021. PMID: 34501286 Free PMC article.
References
-
- Bertelli E., di Gregorio F., Bertelli L., Mosca S. The arterial blood supply of the pancreas: A review. I. The superior pancreaticoduodenal and the anterior superior pancreaticoduodenal arteries. An anatomical and radiological study. Surg. Radiol. Anat. 1995;17:97–106. doi: 10.1007/BF01627566. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
