

Myositis-Related Interstitial Lung Disease: A Respiratory Physician's Point of View
- PMID: 34200737
- PMCID: PMC8230365
- DOI: 10.3390/medicina57060599
Myositis-Related Interstitial Lung Disease: A Respiratory Physician's Point of View
Abstract
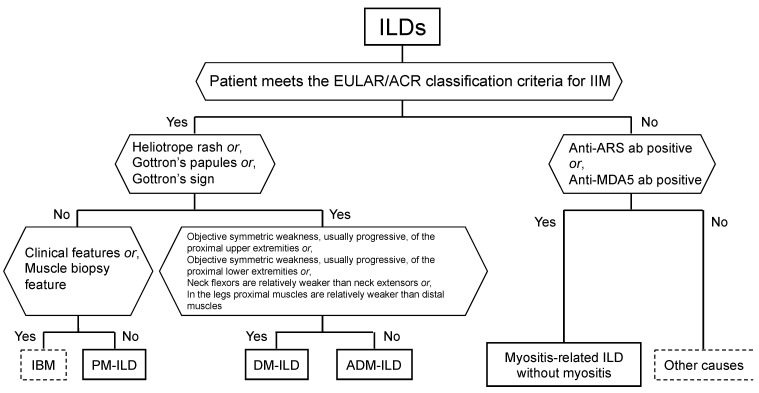
Idiopathic inflammatory myositis (IIM) is an umbrella term for diseases of unknown origin that cause muscle inflammation. Dermatomyositis and polymyositis are IIMs that commonly cause interstitial lung disease (ILD). When a patient presents with ILD, the evaluation of whether the case displays the characteristics of myositis should be determined by interview, physical examination, imaging findings, the measurement of myositis-related antibodies, and the determination of disease severity after diagnosis. Rapidly progressing anti-melanoma differentiation-associated gene 5 antibody-positive ILD may require rapid multi-drug therapy, while anti-aminoacyl tRNA synthetase (ARS) antibody-positive ILD can be treated with anti-inflammatory drugs. Importantly, however, anti-ARS antibody-positive ILD often recurs and sometimes develops into fibrosis. Early diagnosis is crucial for treatment, and we therefore need to clarify the features of myositis associated with ILD and suspect these pathologies early. This section reviews what clinicians need to look for and what findings are evaluated in patients when diagnosing myositis associated with ILD.
Keywords: anti-ARS antibody; anti-MDA5 antibody; dermatomyositis; polymyositis; progressive fibrosing interstitial lung disease; rapid progressive interstitial lung disease.
Conflict of interest statement
Yuko Waseda has received honoraria from Nippon Boehringer Ingelheim for lectures.
Figures


References
-
- Yoshifuji H., Fujii T., Kobayashi S., Imura Y., Fujita Y., Kawabata D., Usui T., Tanaka M., Nagai S., Umehara H., et al. Anti-aminoacyl-tRNA synthetase antibodies in clinical course prediction of interstitial lung disease com-plicated with idiopathic inflammatory myopathies. Autoimmunity. 2006;39:233–241. doi: 10.1080/08916930600622884. - DOI - PubMed
-
- Tsuji H., Nakashima R., Hosono Y., Imura Y., Yagita M., Yoshifuji H., Hirata S., Nojima T., Sugiyama E., Hatta K., et al. Multicenter prospective study of the efficacy and safety of combined immunosuppressive therapy with high-dose glucocorticoid, tacrolimus, and cyclophosphamide in interstitial lung diseases accompanied by anti-melanoma differentiation-associated gene 5-positive dermatomyositis. Arthritis Rheumatol. 2019;72:488–498. - PubMed
-
- Yamasaki Y., Yamada H., Ohkubo M., Yamasaki M., Azuma K., Ogawa H., Mizushima M., Ozaki S. Longterm survival and associated risk factors in patients with adult-onset idiopathic inflammatory myo-pathies and amyopathic dermatomyositis: Experience in a single institute in Japan. J. Rheumatol. 2011;38:1636–1643. doi: 10.3899/jrheum.101002. - DOI - PubMed
-
- Bottai M., Tjärnlund A., Santoni G., Werth V.P., Pilkington C., Visser M., Alfredsson L., Amato A.A., Barohn R.J., Liang M.H., et al. EULAR/ACR classification criteria for adult and juvenile idiopathic inflammatory myopathies and their ma-jor subgroups: A methodology report. Ann. RMD Open. 2017;3:e000507. doi: 10.1136/rmdopen-2017-000507. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
