

A Comprehensive Review of Almond Clinical Trials on Weight Measures, Metabolic Health Biomarkers and Outcomes, and the Gut Microbiota
- PMID: 34201139
- PMCID: PMC8229803
- DOI: 10.3390/nu13061968
A Comprehensive Review of Almond Clinical Trials on Weight Measures, Metabolic Health Biomarkers and Outcomes, and the Gut Microbiota
Abstract
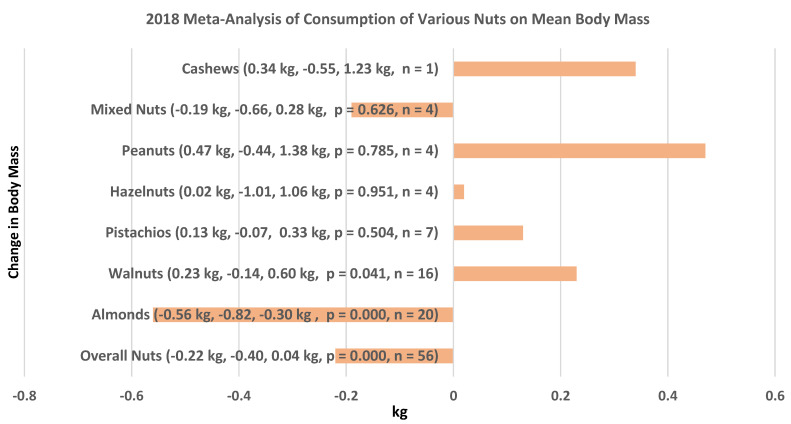
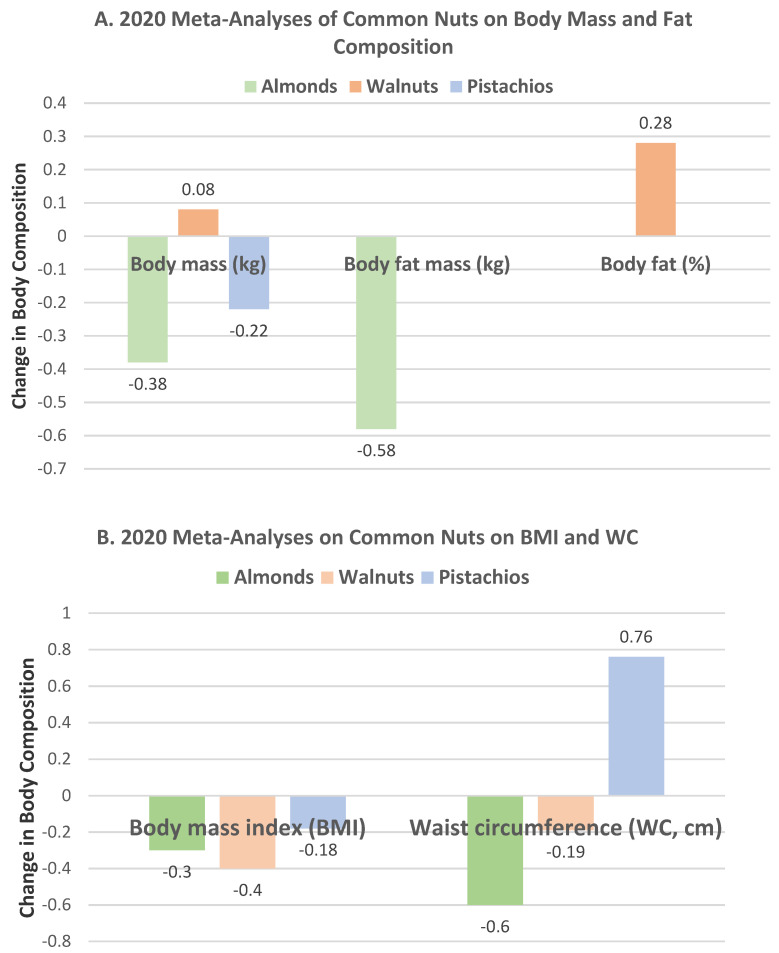
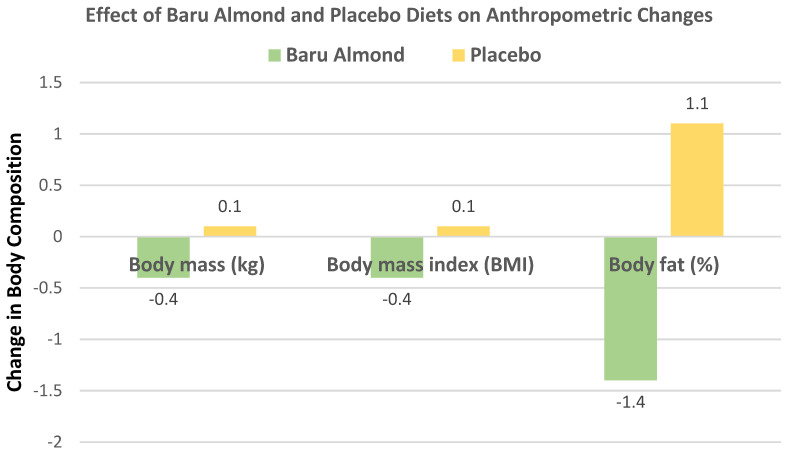
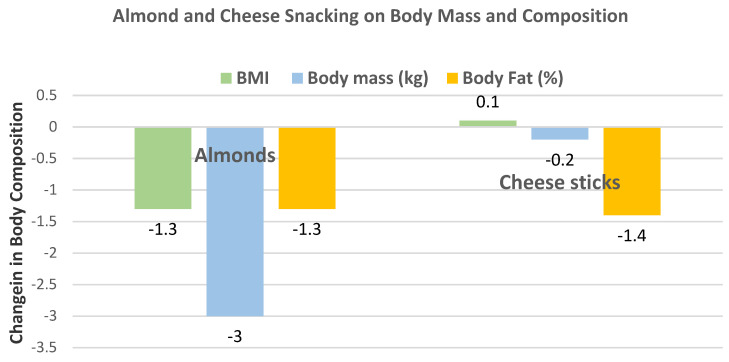
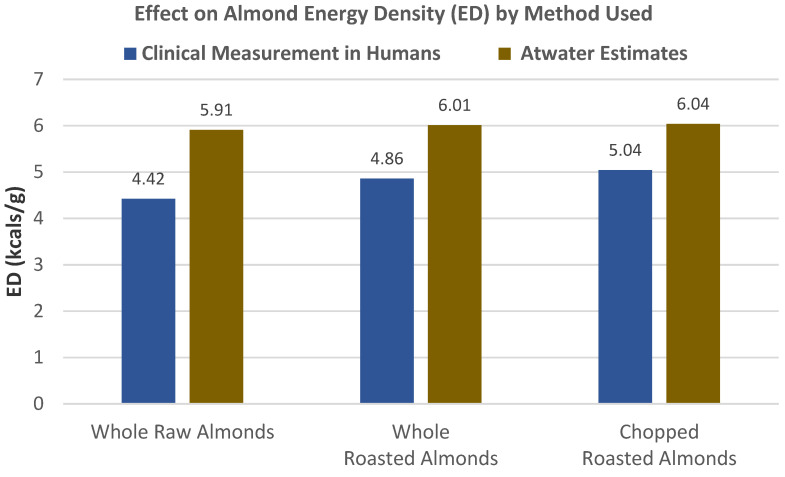
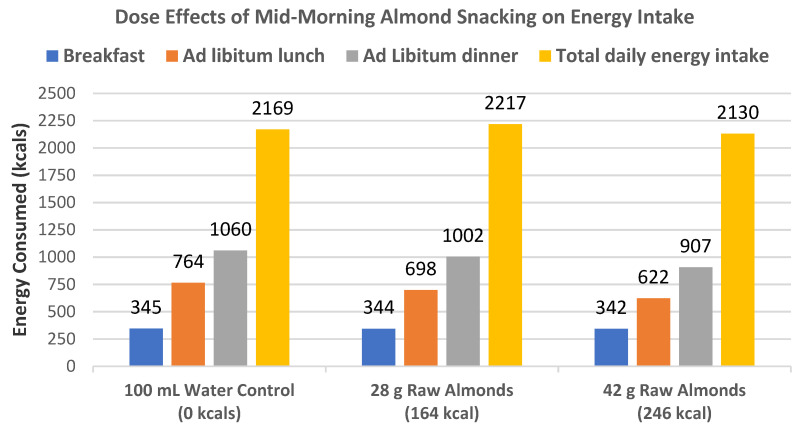
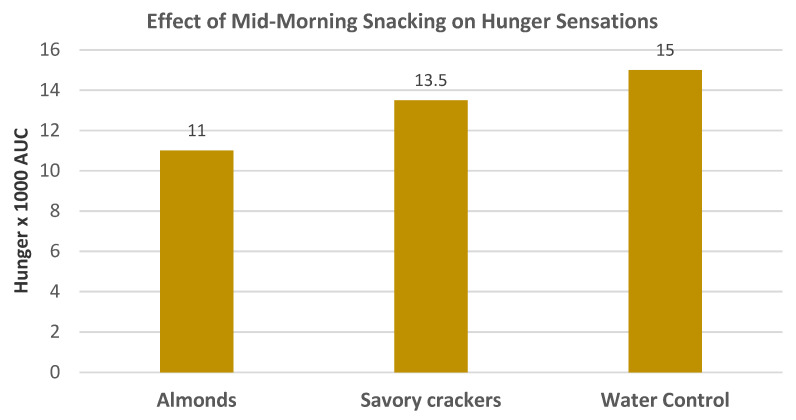
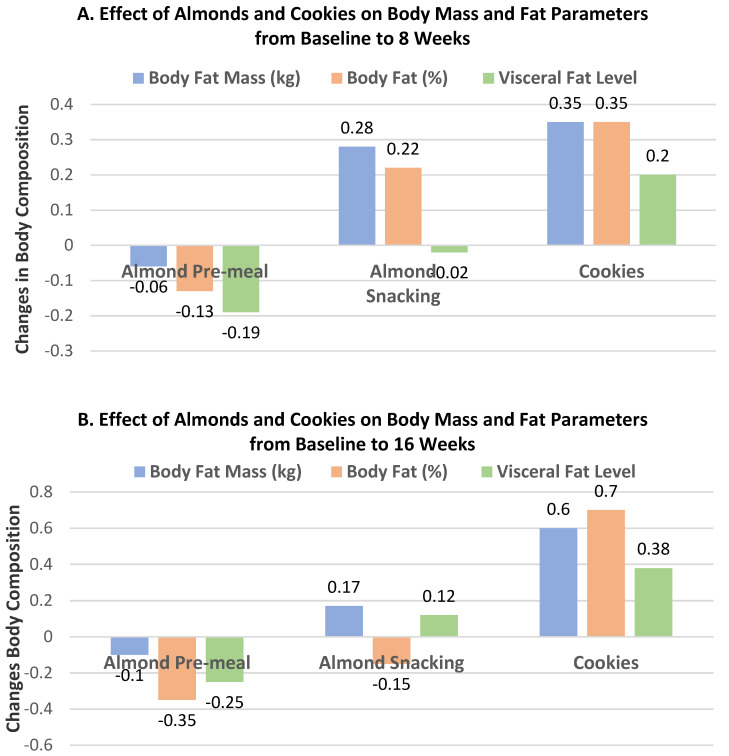
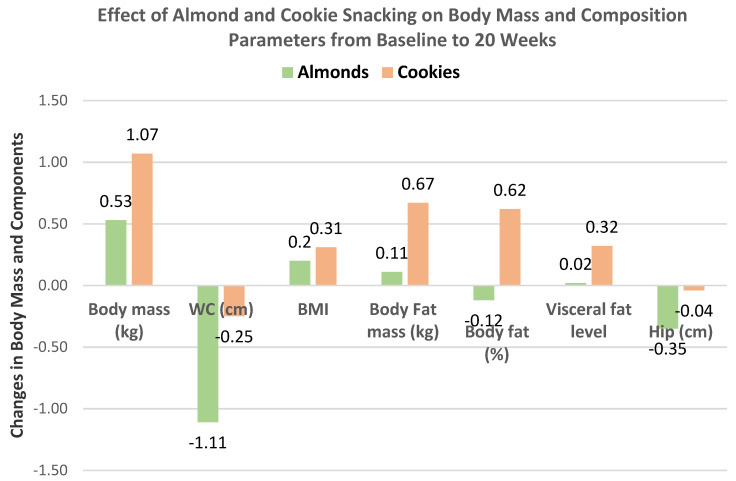
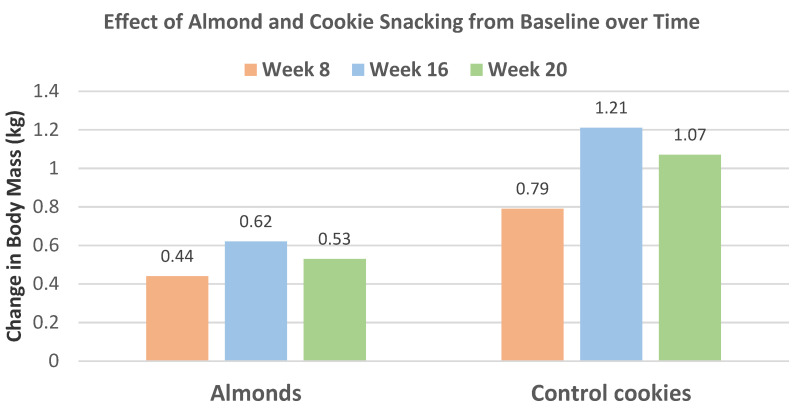
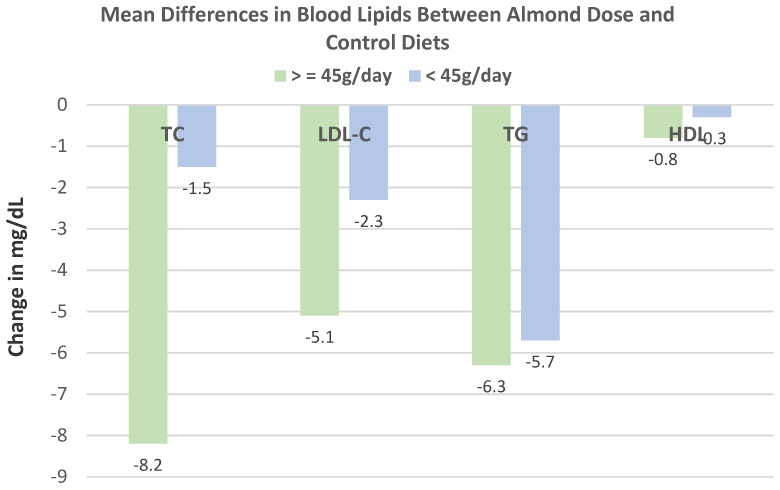
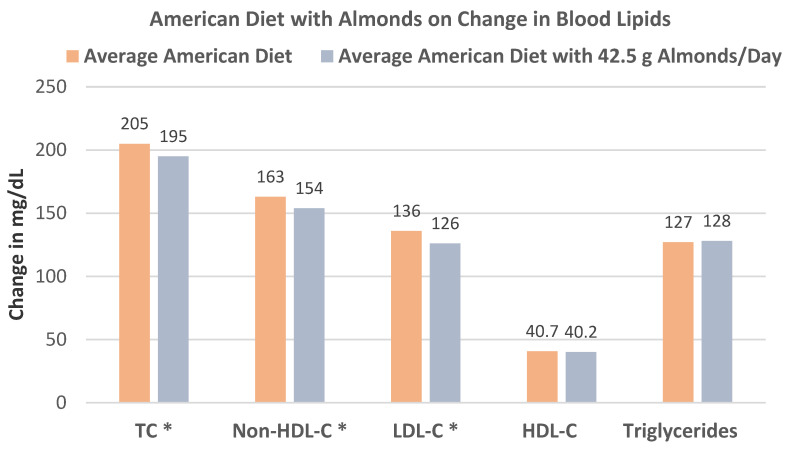
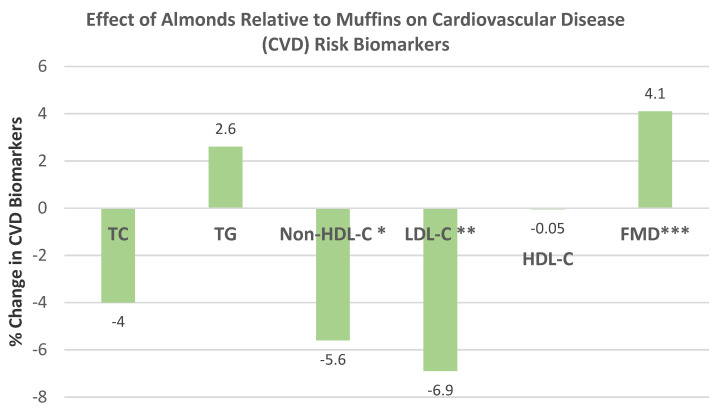
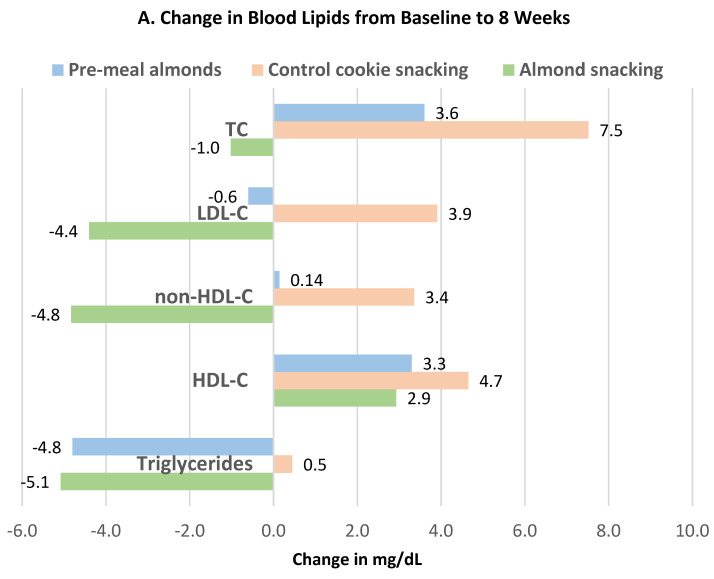
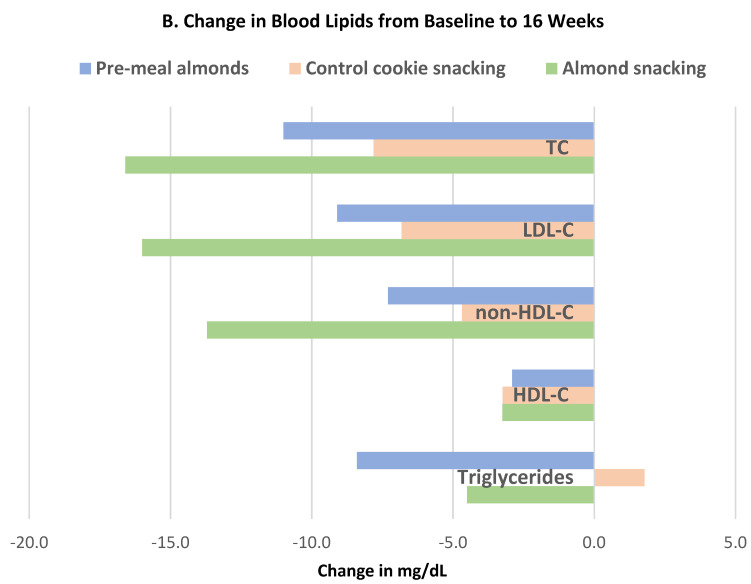
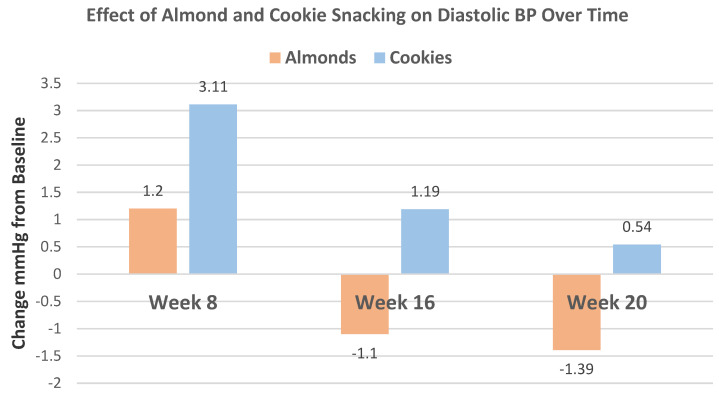
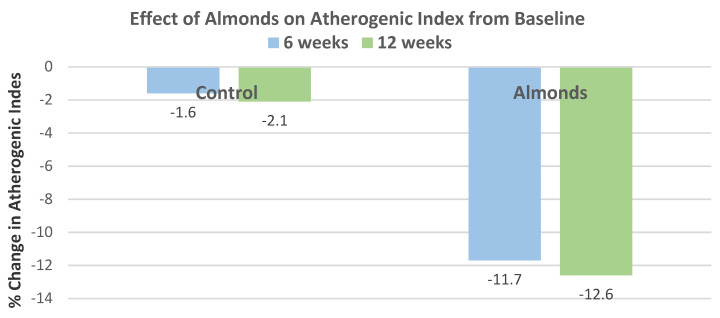
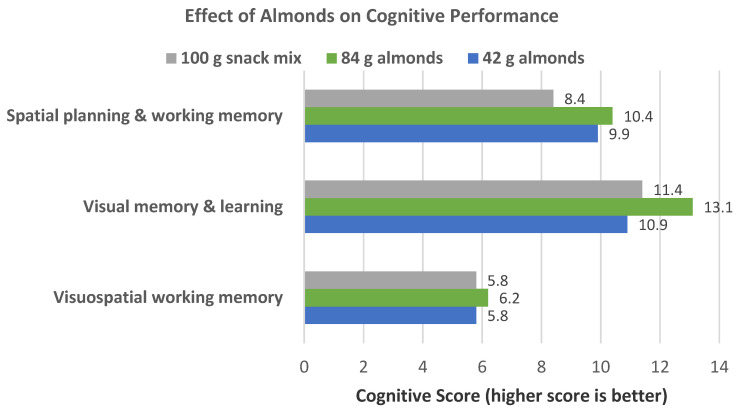
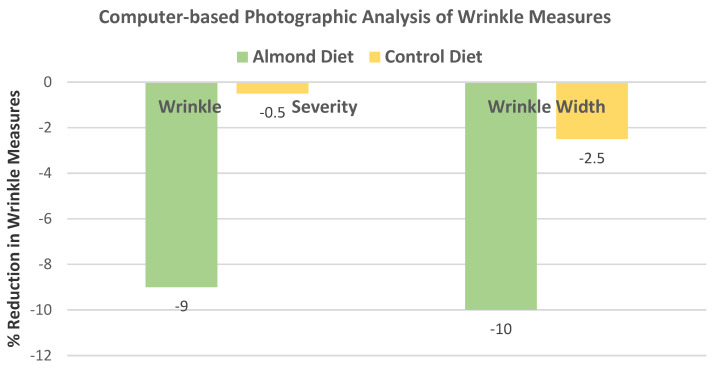
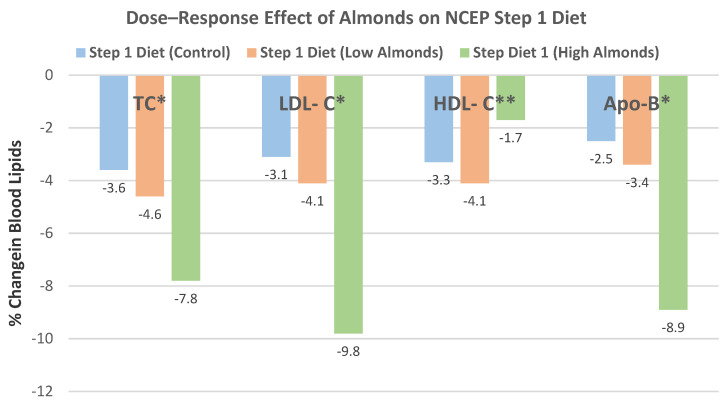
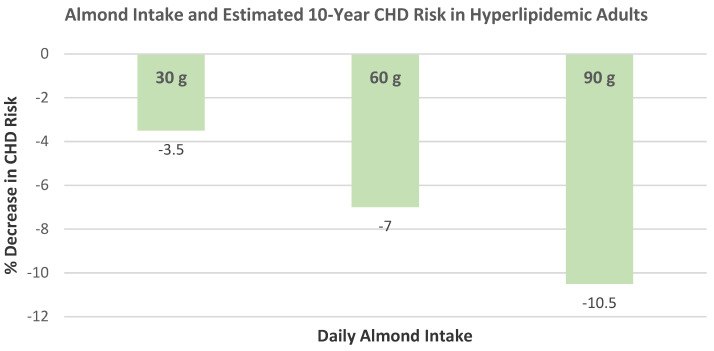
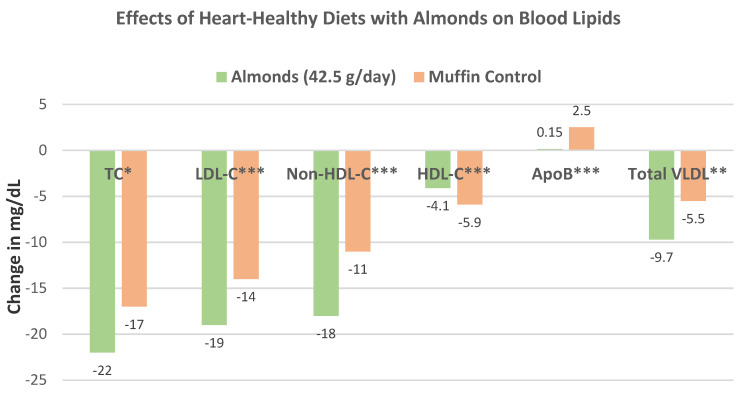
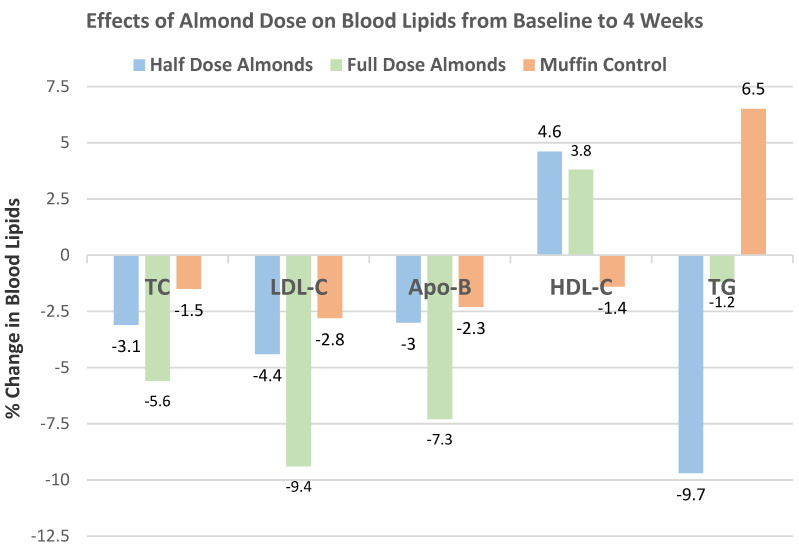
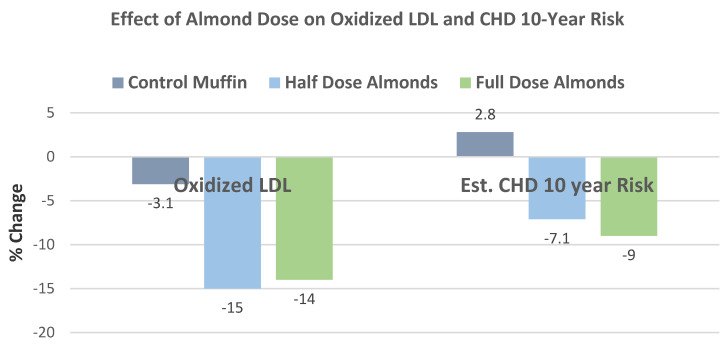
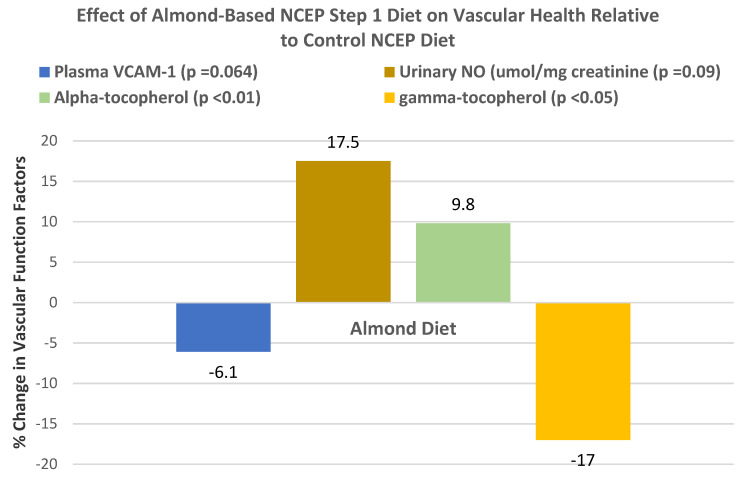
This comprehensive narrative review of 64 randomized controlled trials (RCTs) and 14 systematic reviews and/or meta-analyses provides an in-depth analysis of the effect of almonds on weight measures, metabolic health biomarkers and outcomes, and the colonic microbiota, with extensive use of figures and tables. Almonds are a higher energy-dense (ED) food that acts like a lower ED food when consumed. Recent systematic reviews and meta-analyses of nut RCTs showed that almonds were the only nut that had a small but significant decrease in both mean body mass and fat mass, compared to control diets. The biological mechanisms for almond weight control include enhanced displacement of other foods, decreased macronutrient bioavailability for a lower net metabolizable energy (ME), upregulation of acute signals for reduced hunger, and elevated satiety and increased resting energy expenditure. The intake of 42.5 g/day of almonds significantly lowered low-density lipoprotein cholesterol (LDL-C), 10-year Framingham estimated coronary heart disease (CHD) risk and associated cardiovascular disease (CVD) medical expenditures. Diastolic blood pressure (BP) was modestly but significantly lowered when almonds were consumed at >42.5 g/day or for >6 weeks. Recent RCTs suggest possible emerging health benefits for almonds such as enhanced cognitive performance, improved heart rate variability under mental stress, and reduced rate of facial skin aging from exposure to ultraviolet (UV) B radiation. Eight RCTs show that almonds can support colonic microbiota health by promoting microflora richness and diversity, increasing the ratio of symbiotic to pathogenic microflora, and concentrations of health-promoting colonic bioactives. Almonds are a premier healthy snack for precision nutrition diet plans.
Keywords: almonds; blood lipids; blood pressure (BP); body fat % (BF%); body mass; body mass index (BMI); body weight; central obesity; cognitive performance; colonic microbiota; coronary heart disease (CHD); endothelial health; energy density (ED); fat mass (FM); fat-free mass (FFM); glycemic control; hs-C-reactive protein (hs-CRP); insulin sensitivity; low-calorie diets (LCDs); nuts; pre-diabetes; precision nutrition; type 2 (T2) diabetes; waist circumference (WC).
Conflict of interest statement
M.L.D. is an ad hoc nutrition research consultant and was a voluntary member of the Almond Board of California’s Nutrition Research Committee from 2006 to 2018. There was no input from this Committee in the writing of this manuscript.
Figures
References
-
- U.S. Department of Agriculture, Agricultural Research Service Food Data Central, Almond Legacy. [(accessed on 18 November 2020)];2019 Available online: fdc.nal.usda.gov.
-
- Dikariyanto V., Berry S.E., Francis L., Smith L., Hall W.L. Whole almond consumption is associated with better diet quality and cardiovascular disease risk factors in the UK adult population: National Diet and Nutrition Survey (NDNS) 2008–2017. Eur. J Nutr. 2020;60:643–654. doi: 10.1007/s00394-020-02270-9. - DOI - PMC - PubMed
-
- Mattes R.D., Dreher M.L. Nuts and healthy body weight maintenance mechanisms. Asia Pac. J. Clin. Nutr. 2010;19:137–141. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
