

OCT Findings in MINOCA
- PMID: 34201727
- PMCID: PMC8269308
- DOI: 10.3390/jcm10132759
OCT Findings in MINOCA
Abstract
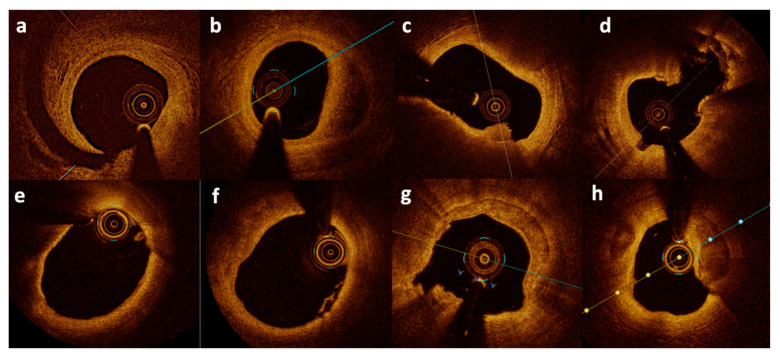
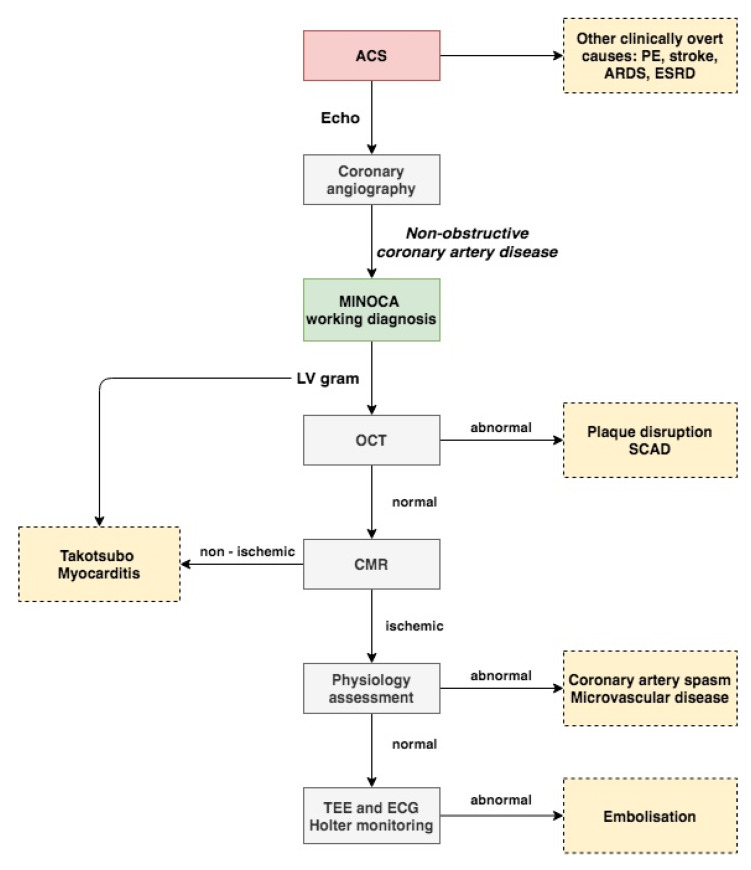
Myocardial infarction with non-obstructive coronary artery disease (MINOCA) is a working diagnosis for patients presenting with acute myocardial infarction without obstructive coronary artery disease on coronary angiography. It is a heterogenous entity with a number of possible etiologies that can be determined through the use of appropriate diagnostic algorithms. Common causes of a MINOCA may include plaque disruption, spontaneous coronary artery dissection, coronary artery spasm, and coronary thromboembolism. Optical coherence tomography (OCT) is an intravascular imaging modality which allows the differentiation of coronary tissue morphological characteristics including the identification of thin cap fibroatheroma and the differentiation between plaque rupture or erosion, due to its high resolution. In this narrative review we will discuss the role of OCT in patients presenting with MINOCA. In this group of patients OCT has been shown to reveal abnormal findings in almost half of the cases. Moreover, combining OCT with cardiac magnetic resonance (CMR) was shown to allow the identification of most of the underlying mechanisms of MINOCA. Hence, it is recommended that both OCT and CMR can be used in patients with a working diagnosis of MINOCA. Well-designed prospective studies are needed in order to gain a better understanding of this condition and to provide optimal management while reducing morbidity and mortality in that subset patients.
Keywords: acute myocardial infarction; cardiovascular disease; intravascular imaging.
Conflict of interest statement
Jang’s research was supported by the Allan Gray Fellowship Fund and by Michael and Kathryn Park. Jang has received educational grants from Abbott Vascular and a consulting fee from Svelte Medical Systems Inc. (NJ, USA) and Mitobridge Inc. (MA, USA).
Figures
Similar articles
-
[Cardiac magnetic resonance imaging and coronary optical coherence tomography : Acquisition techniques, interpretation and integration in diagnostic algorithms for MINOCA].Ann Cardiol Angeiol (Paris). 2022 Dec;71(6):381-390. doi: 10.1016/j.ancard.2022.09.006. Epub 2022 Oct 20. Ann Cardiol Angeiol (Paris). 2022. PMID: 36273952 Review. French.
-
OCT and CMR for the Diagnosis of Patients Presenting With MINOCA and Suspected Epicardial Causes.JACC Cardiovasc Imaging. 2020 Dec;13(12):2619-2631. doi: 10.1016/j.jcmg.2020.05.045. Epub 2020 Aug 19. JACC Cardiovasc Imaging. 2020. PMID: 32828786
-
Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women.Circulation. 2021 Feb 16;143(7):624-640. doi: 10.1161/CIRCULATIONAHA.120.052008. Epub 2020 Nov 14. Circulation. 2021. PMID: 33191769 Free PMC article.
-
Role of Intracoronary Imaging in Myocardial Infarction with Non-Obstructive Coronary Disease (MINOCA): A Review.J Clin Med. 2023 Mar 8;12(6):2129. doi: 10.3390/jcm12062129. J Clin Med. 2023. PMID: 36983131 Free PMC article. Review.
-
Optical coherence tomography in the diagnosis of myocardial infarction with non-obstructive coronary arteries.Postepy Kardiol Interwencyjnej. 2022 Sep;18(3):192-200. doi: 10.5114/aic.2022.121233. Epub 2022 Nov 19. Postepy Kardiol Interwencyjnej. 2022. PMID: 36751279 Free PMC article. Review.
Cited by
-
Management of Residual Risk in Chronic Coronary Syndromes. Clinical Pathways for a Quality-Based Secondary Prevention.J Clin Med. 2023 Sep 15;12(18):5989. doi: 10.3390/jcm12185989. J Clin Med. 2023. PMID: 37762932 Free PMC article. Review.
-
Myocardial Infarction With Non-obstructive Coronary Arteries (MINOCA): A Case Report and Comprehensive Discussion of Pathophysiology and Risk Factors.Cureus. 2024 Aug 18;16(8):e67144. doi: 10.7759/cureus.67144. eCollection 2024 Aug. Cureus. 2024. PMID: 39161551 Free PMC article.
-
Emotional Stress Induced Broken Heart Syndrome: A Case Report.Cureus. 2022 Dec 10;14(12):e32384. doi: 10.7759/cureus.32384. eCollection 2022 Dec. Cureus. 2022. PMID: 36632256 Free PMC article.
-
Use of Optical Coherence Tomography in MI with Non-obstructive Coronary Arteries.Interv Cardiol. 2022 May 9;17:e06. doi: 10.15420/icr.2021.31. eCollection 2022 Jan. Interv Cardiol. 2022. PMID: 35602588 Free PMC article. Review.
-
Intracoronary Imaging of Vulnerable Plaque-From Clinical Research to Everyday Practice.J Clin Med. 2022 Nov 9;11(22):6639. doi: 10.3390/jcm11226639. J Clin Med. 2022. PMID: 36431116 Free PMC article. Review.
References
-
- Bean W.B. Infarction of the heart. III. clinical course and morphological findings. Ann. Intern. Med. 1938;12:71–94.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
