

Coinfections with Bacteria, Fungi, and Respiratory Viruses in Patients with SARS-CoV-2: A Systematic Review and Meta-Analysis
- PMID: 34202114
- PMCID: PMC8308492
- DOI: 10.3390/pathogens10070809
Coinfections with Bacteria, Fungi, and Respiratory Viruses in Patients with SARS-CoV-2: A Systematic Review and Meta-Analysis
Abstract
Background: Coinfection with bacteria, fungi, and respiratory viruses in SARS-CoV-2 is of particular importance due to the possibility of increased morbidity and mortality. In this meta-analysis, we calculated the prevalence of such coinfections.
Methods: Electronic databases were searched from 1 December 2019 to 31 March 2021. Effect sizes of prevalence were pooled with 95% confidence intervals (CIs). To minimize heterogeneity, we performed sub-group analyses.
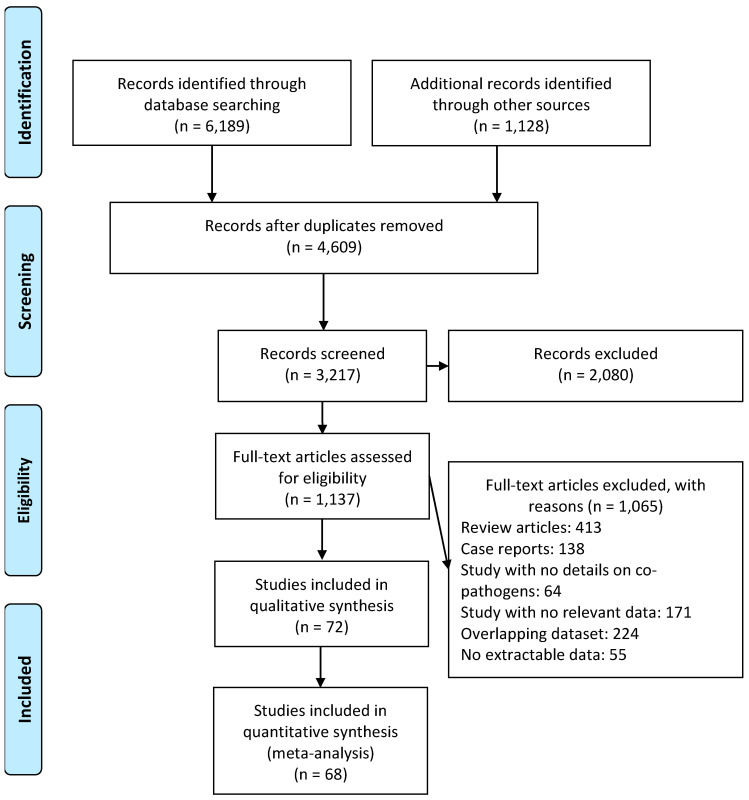
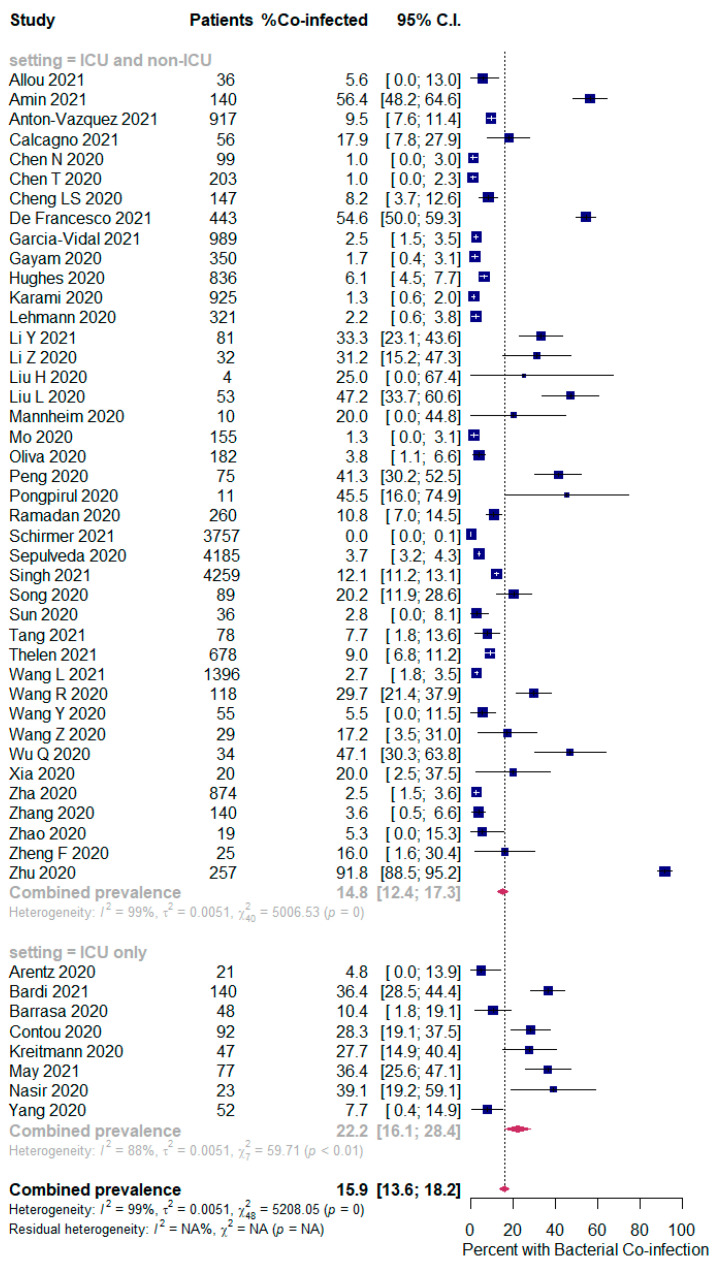
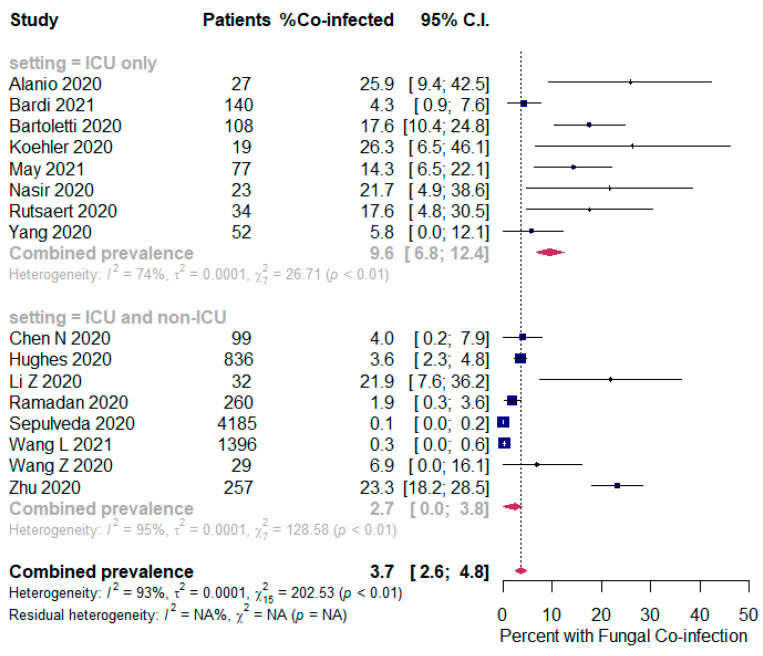
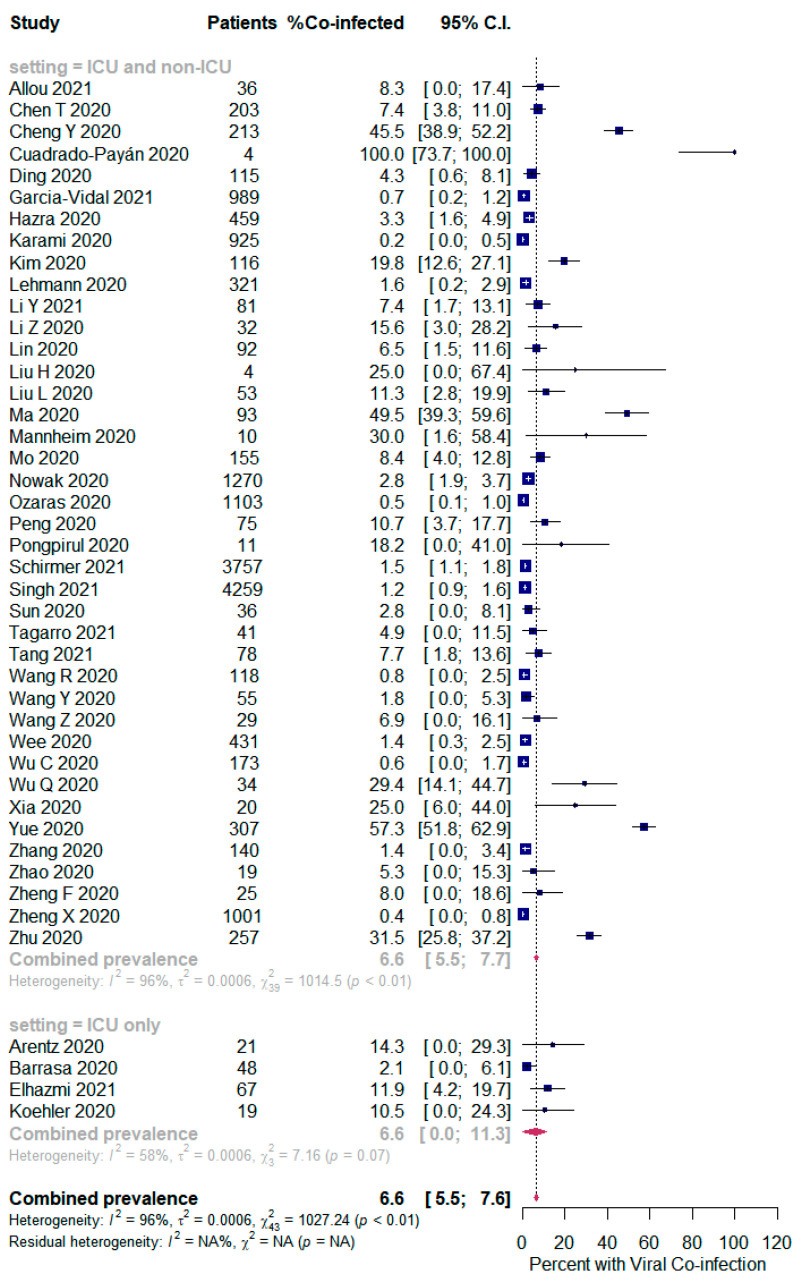
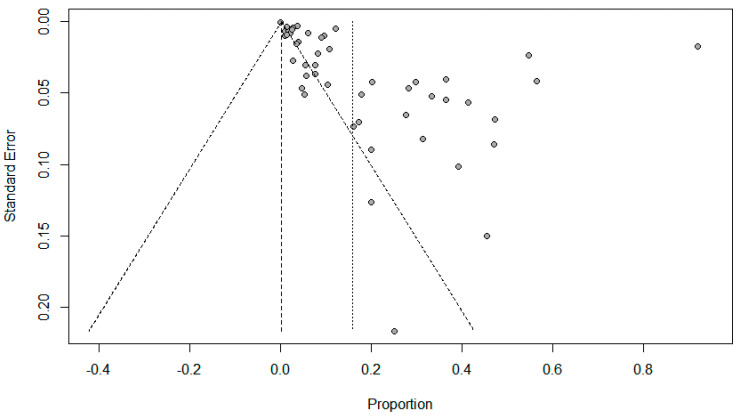
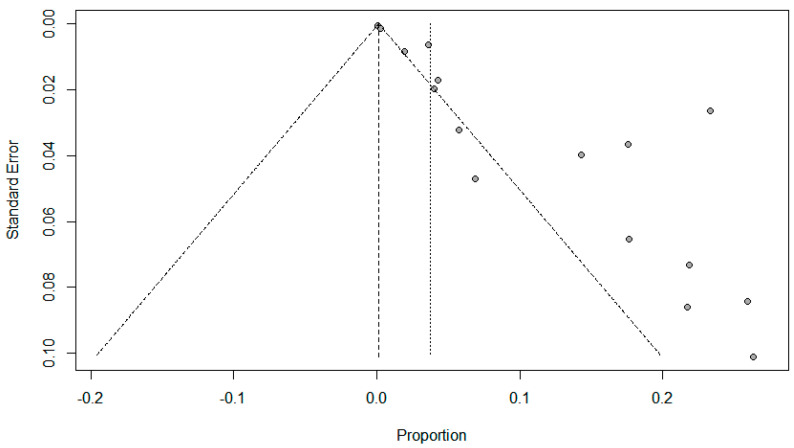
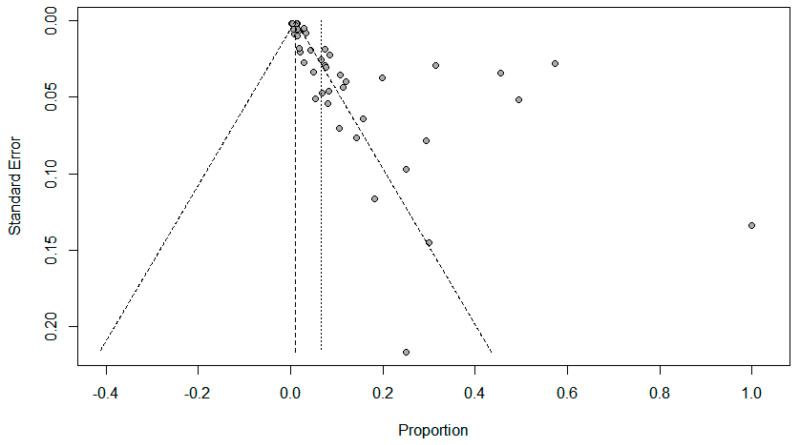
Results: Of the 6189 papers that were identified, 72 articles were included in the systematic review (40 case series and 32 cohort studies) and 68 articles (38 case series and 30 cohort studies) were included in the meta-analysis. Of the 31,953 SARS-CoV-2 patients included in the meta-analysis, the overall pooled proportion who had a laboratory-confirmed bacterial infection was 15.9% (95% CI 13.6-18.2, n = 1940, 49 studies, I2 = 99%, p < 0.00001), while 3.7% (95% CI 2.6-4.8, n = 177, 16 studies, I2 = 93%, p < 0.00001) had fungal infections and 6.6% (95% CI 5.5-7.6, n = 737, 44 studies, I2 = 96%, p < 0.00001) had other respiratory viruses. SARS-CoV-2 patients in the ICU had higher co-infections compared to ICU and non-ICU patients as follows: bacterial (22.2%, 95% CI 16.1-28.4, I2 = 88% versus 14.8%, 95% CI 12.4-17.3, I2 = 99%), and fungal (9.6%, 95% CI 6.8-12.4, I2 = 74% versus 2.7%, 95% CI 0.0-3.8, I2 = 95%); however, there was an identical other respiratory viral co-infection proportion between all SARS-CoV-2 patients [(ICU and non-ICU) and the ICU only] (6.6%, 95% CI 0.0-11.3, I2 = 58% versus 6.6%, 95% CI 5.5-7.7, I2 = 96%). Funnel plots for possible publication bias for the pooled effect sizes of the prevalence of coinfections was asymmetrical on visual inspection, and Egger's tests confirmed asymmetry (p values < 0.05).
Conclusion: Bacterial co-infection is relatively high in hospitalized patients with SARS-CoV-2, with little evidence of S. aureus playing a major role. Knowledge of the prevalence and type of co-infections in SARS-CoV-2 patients may have diagnostic and management implications.
Keywords: COVID-19; SARS-Cov-2; bacterial; co-infection; coinfection; concurrent; fungal; meta-analysis; viral.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization WHO Coronavirus (COVID-19) Dashboard. [(accessed on 5 April 2021)];2021 Available online: https://covid19.who.int.
-
- Bardi T., Pintado V., Gomez-Rojo M., Escudero-Sanchez R., Lopez A.A., Diez-Remesal Y., Castro N.M., Ruiz-Garbajosa P., Pestaña D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021;40:495–502. doi: 10.1007/s10096-020-04142-w. - DOI - PMC - PubMed
-
- May A., Swetenham N., Pandey M., Taylor V., Hughes H., Underwood J. P197 Bacterial and fungal respiratory co-infection among patients admitted to ICU with COVID-19: A retrospective cohort study in a UK hospital. BMJ. 2021;76:A196–A197.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
