

Re-Irradiation for Head and Neck Cancer: Cumulative Dose to Organs at Risk and Late Side Effects
- PMID: 34202135
- PMCID: PMC8269009
- DOI: 10.3390/cancers13133173
Re-Irradiation for Head and Neck Cancer: Cumulative Dose to Organs at Risk and Late Side Effects
Abstract
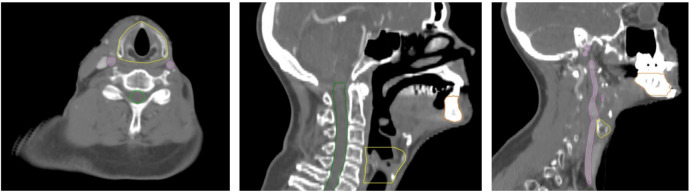
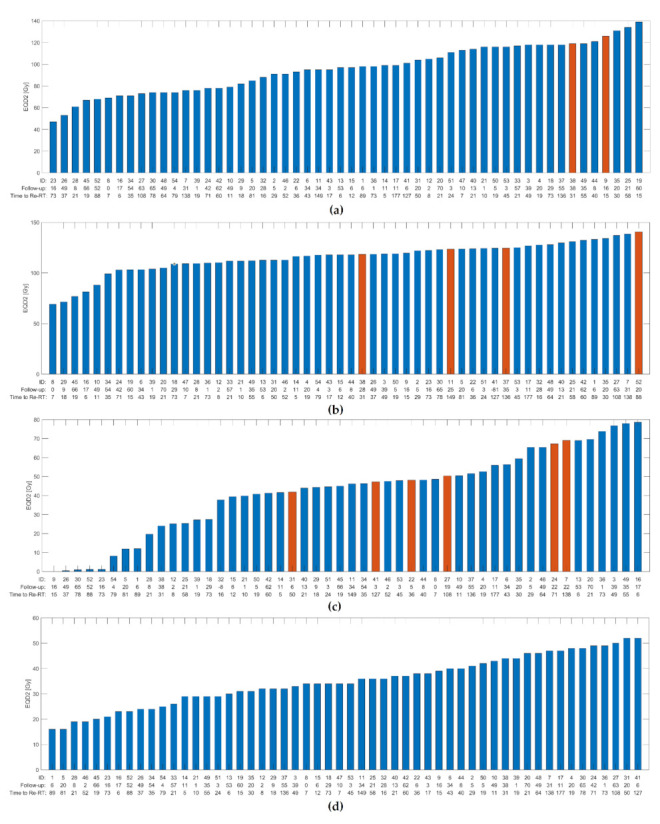
Re-irradiation in head and neck cancer is challenging, and cumulative dose constraints and dose/volume data are scarce. In this study, we present dose/volume data for patients re-irradiated for head and neck cancer and explore the correlations of cumulative dose to organs at risk and severe side effects. We analyzed 54 patients re-irradiated for head and neck cancer between 2011 and 2017. Organs at risk were delineated and dose/volume data were collected from cumulative treatment plans of all included patients. Receiver-operator characteristics (ROC) analysis assessed the association between dose/volume parameters and the risk of toxicity. The ROC-curve for a logistic model of carotid blowout vs. maximum doses to the carotid arteries showed AUC = 0.92 (95% CI 0.83 to 1.00) and a cut-off value of 119 Gy (sensitivity 1.00/specificity 0.89). The near-maximum dose to bones showed an association with the risk of osteoradionecrosis: AUC = 0.74 (95% CI 0.52 to 0.95) and a cut-off value of 119 Gy (sensitivity 1.00/specificity 0.52). Our analysis showed an association between cumulative dose to organs at risk and the risk of developing osteoradionecrosis and carotid blowout, and our results support the existing dose constraint for the carotid arteries of 120 Gy. The confirmation of these dose-response relationships will contribute to further improvements of re-irradiation strategies.
Keywords: carotid blowout; composite DVH; cumulative dose; head and neck cancer; late side effects; organs at risk; osteoradionecrosis; re-irradiation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Overgaard J., Hansen H.S., Specht L., Overgaard M., Grau C., Andersen E., Bentzen J., Bastholt L., Hansen O., Johansen J., et al. Five compared with six fractions per week of conventional radiotherapy of squamous-cell carcinoma of head and neck: DAHANCA 6 and 7 randomised controlled trial. Lancet. 2003;362:933–940. doi: 10.1016/S0140-6736(03)14361-9. - DOI - PubMed
-
- Ward M.C., Riaz N., Caudell J.J., Dunlap N.E., Isrow D., Zakem S.J., Dault J., Awan M.J., Vargo J.A., Heron D.E., et al. Refining Patient Selection for Reirradiation of Head and Neck Squamous Carcinoma in the IMRT Era: A Multi-institution Cohort Study by the MIRI Collaborative. Int. J. Radiat. Oncol. Biol. Phys. 2018;100:586–594. doi: 10.1016/j.ijrobp.2017.06.012. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
