

Centromedian-Parafascicular and Somatosensory Thalamic Deep Brain Stimulation for Treatment of Chronic Neuropathic Pain: A Contemporary Series of 40 Patients
- PMID: 34202202
- PMCID: PMC8301341
- DOI: 10.3390/biomedicines9070731
Centromedian-Parafascicular and Somatosensory Thalamic Deep Brain Stimulation for Treatment of Chronic Neuropathic Pain: A Contemporary Series of 40 Patients
Abstract
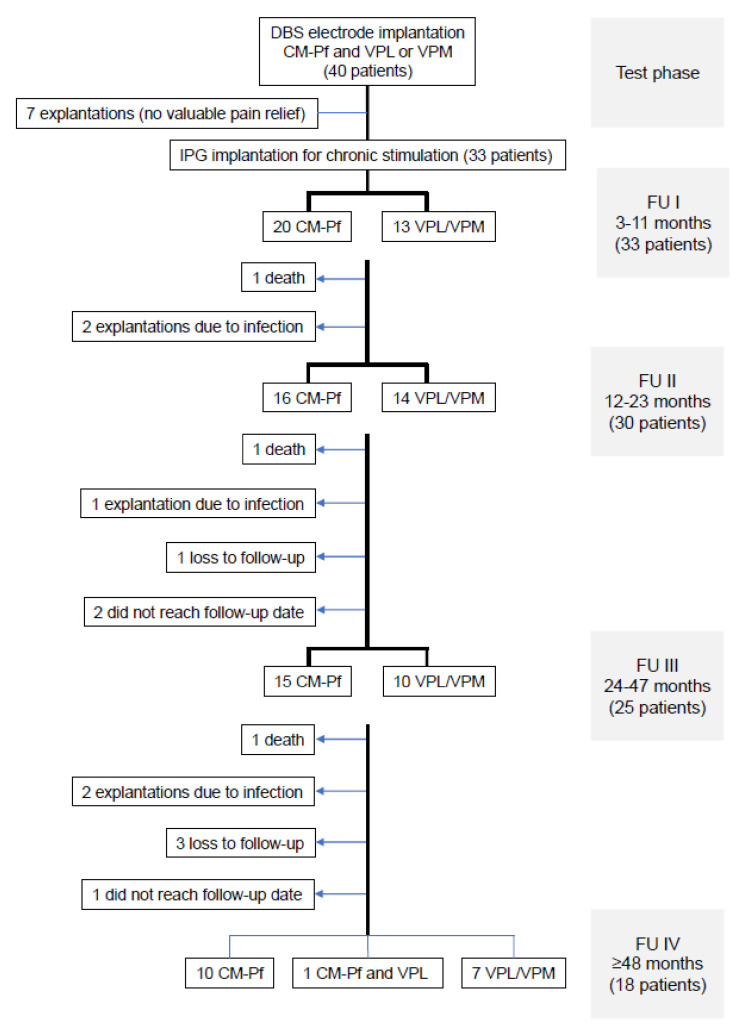
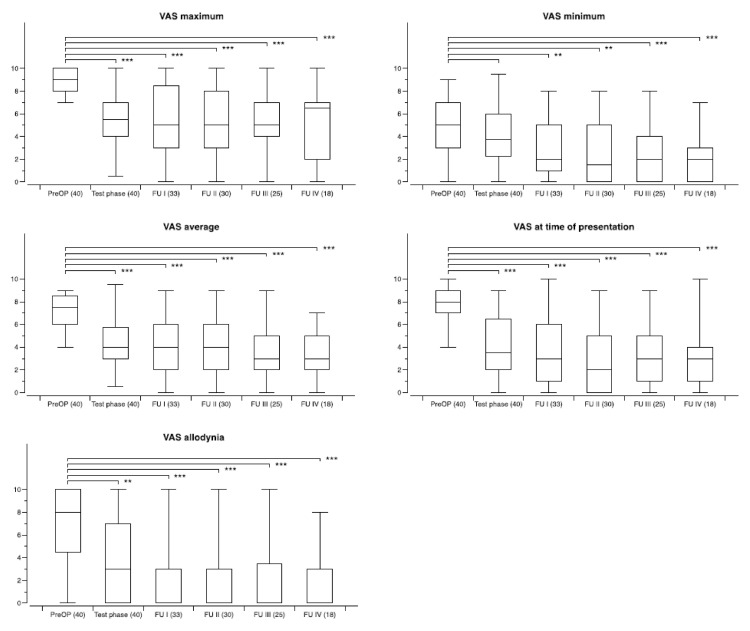
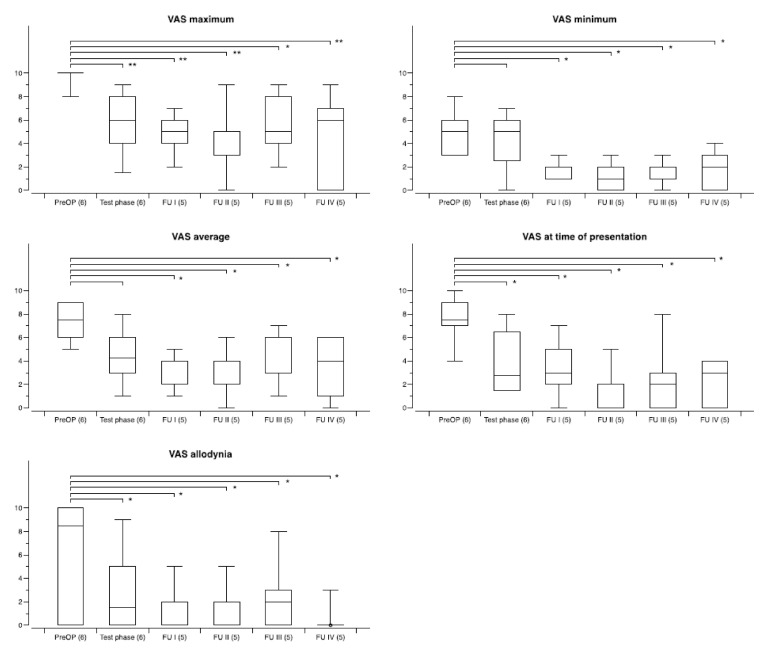
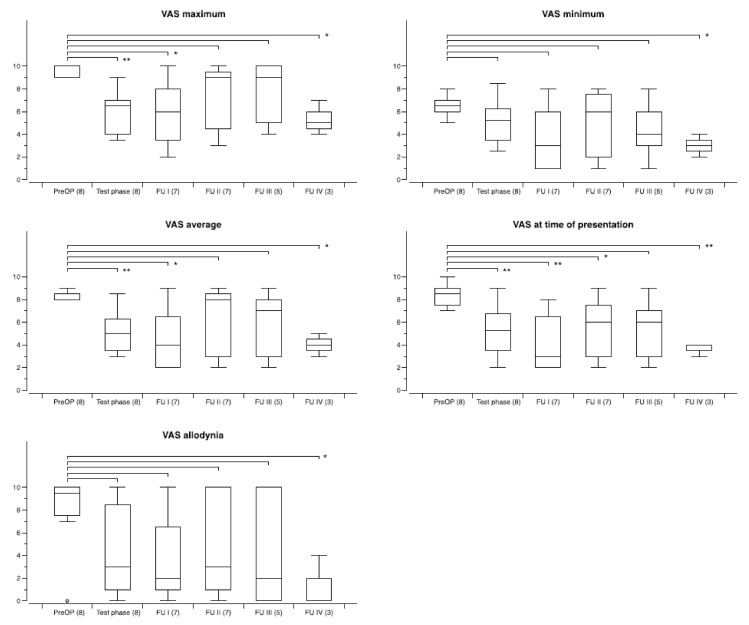
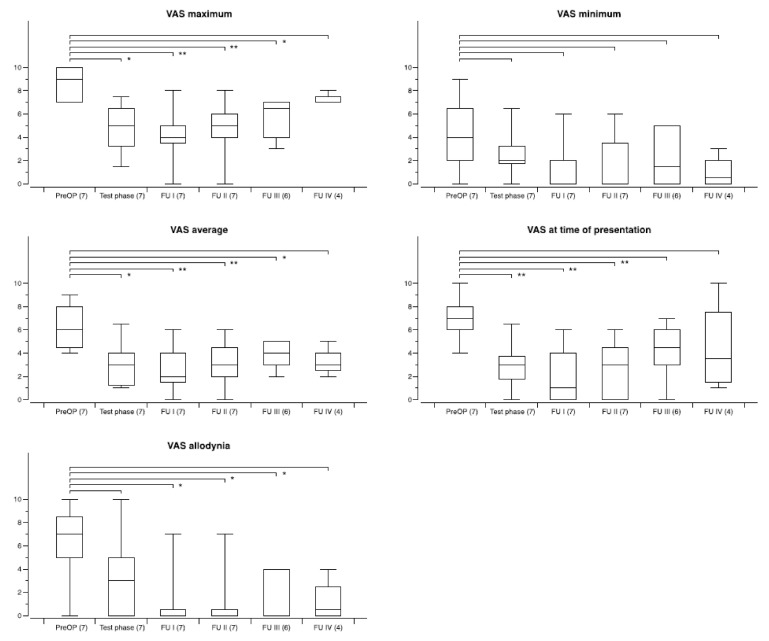
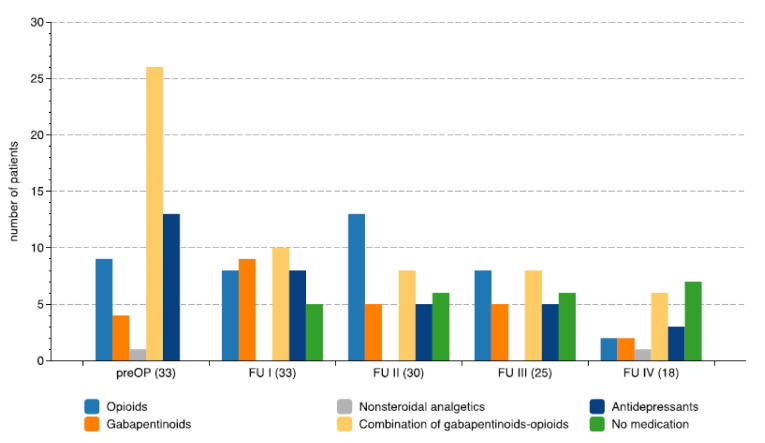
Introduction: The treatment of neuropathic and central pain still remains a major challenge. Thalamic deep brain stimulation (DBS) involving various target structures is a therapeutic option which has received increased re-interest. Beneficial results have been reported in several more recent smaller studies, however, there is a lack of prospective studies on larger series providing long term outcomes. Methods: Forty patients with refractory neuropathic and central pain syndromes underwent stereotactic bifocal implantation of DBS electrodes in the centromedian-parafascicular (CM-Pf) and the ventroposterolateral (VPL) or ventroposteromedial (VPM) nucleus contralateral to the side of pain. Electrodes were externalized for test stimulation for several days. Outcome was assessed with five specific VAS pain scores (maximum, minimum, average pain, pain at presentation, allodynia). Results: The mean age at surgery was 53.5 years, and the mean duration of pain was 8.2 years. During test stimulation significant reductions of all five pain scores was achieved with either CM-Pf or VPL/VPM stimulation. Pacemakers were implanted in 33/40 patients for chronic stimulation for whom a mean follow-up of 62.8 months (range 3-180 months) was available. Of these, 18 patients had a follow-up beyond four years. Hardware related complications requiring secondary surgeries occurred in 11/33 patients. The VAS maximum pain score was improved by ≥50% in 8/18, and by ≥30% in 11/18 on long term follow-up beyond four years, and the VAS average pain score by ≥50% in 10/18, and by ≥30% in 16/18. On a group level, changes in pain scores remained statistically significant over time, however, there was no difference when comparing the efficacy of CM-Pf versus VPL/VPM stimulation. The best results were achieved in patients with facial pain, poststroke/central pain (except thalamic pain), or brachial plexus injury, while patients with thalamic lesions had the least benefit. Conclusion: Thalamic DBS is a useful treatment option in selected patients with severe and medically refractory pain.
Keywords: centromedian–parafascicular complex; deep brain stimulation; functional neurosurgery; pain; ventroposterolateral thalamus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
