

Molecular Subtypes and Precision Oncology in Intrahepatic Cholangiocarcinoma
- PMID: 34202401
- PMCID: PMC8269161
- DOI: 10.3390/jcm10132803
Molecular Subtypes and Precision Oncology in Intrahepatic Cholangiocarcinoma
Abstract
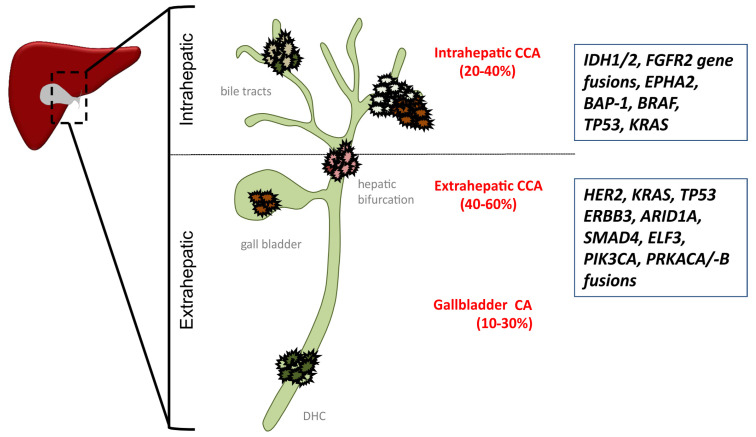
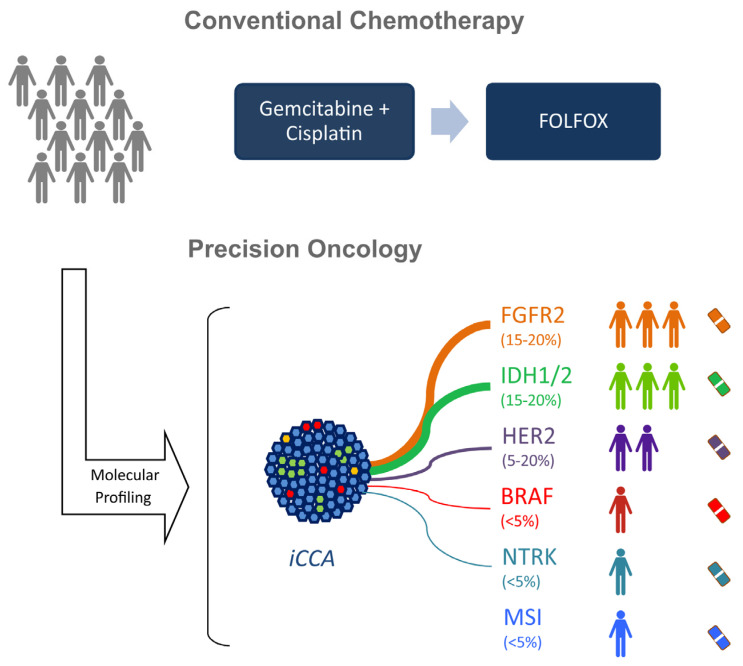
Cholangiocarcinomas (CCAs) are the second-most common primary liver cancers. CCAs represent a group of highly heterogeneous tumors classified based on anatomical localization into intra- (iCCA) and extrahepatic CCA (eCCA). In contrast to eCCA, the incidence of iCCA is increasing worldwide. Curative treatment strategies for all CCAs involve oncological resection followed by adjuvant chemotherapy in early stages, whereas chemotherapy is administered at advanced stages of disease. Due to late diagnosis, high recurrence rates, and limited treatment options, the prognosis of patients remains poor. Comprehensive molecular characterization has further revealed considerable heterogeneity and distinct prognostic and therapeutic traits for iCCA and eCCA, indicating that specific treatment modalities are required for different subclasses. Several druggable alterations and oncogenic drivers such as fibroblast growth factor receptor 2 gene fusions and hotspot mutations in isocitrate dehydrogenase 1 and 2 mutations have been identified. Specific inhibitors have demonstrated striking antitumor activity in affected subgroups of patients in phase II and III clinical trials. Thus, improved understanding of the molecular complexity has paved the way for precision oncological approaches. Here, we outline current advances in targeted treatments and immunotherapeutic approaches. In addition, we delineate future perspectives for different molecular subclasses that will improve the clinical care of iCCA patients.
Keywords: FGFR; IDH1; cholangiocarcinoma; immunotherapy; targeted therapy.
Conflict of interest statement
J.U.M. received honoraria from Roche, Bayer, Ipsen, Merz, AstraZeneca, Johnson & Johnson, MSD, Leap-Tx, and Eisai. A.V. received honoraria as a speaker, consultant, and advisor from Roche, Bayer, Sanofi, BMS, Lilly, Novartis, EISAI, AstraZeneca, Merck, Incyte, Ipsen, PierreFabre, MSD, and Janssen. C.C. reports receiving consulting fees from MSD and lecture fees from EISAI.
Figures
References
-
- van der Gaag N.A., Kloek J.J., de Bakker J.K., Musters B., Geskus R.B., Busch O.R.C., Bosma A., Gouma D.J., van Gulik T.M. Survival analysis and prognostic nomogram for patients undergoing resection of extrahepatic cholangiocarcinoma. Ann. Oncol. 2012;23:2642–2649. doi: 10.1093/annonc/mds077. - DOI - PubMed
-
- Spolverato G., Yakoob M.Y., Kim Y., Alexandrescu S., Marques H.P., Lamelas J., Aldrighetti L., Gamblin T.C., Maithel S.K., Pulitano C., et al. The Impact of Surgical Margin Status on Long-Term Outcome After Resection for Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2015;22:4020–4028. doi: 10.1245/s10434-015-4472-9. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
