

BPC 157 Therapy and the Permanent Occlusion of the Superior Sagittal Sinus in Rat: Vascular Recruitment
- PMID: 34203464
- PMCID: PMC8301421
- DOI: 10.3390/biomedicines9070744
BPC 157 Therapy and the Permanent Occlusion of the Superior Sagittal Sinus in Rat: Vascular Recruitment
Abstract
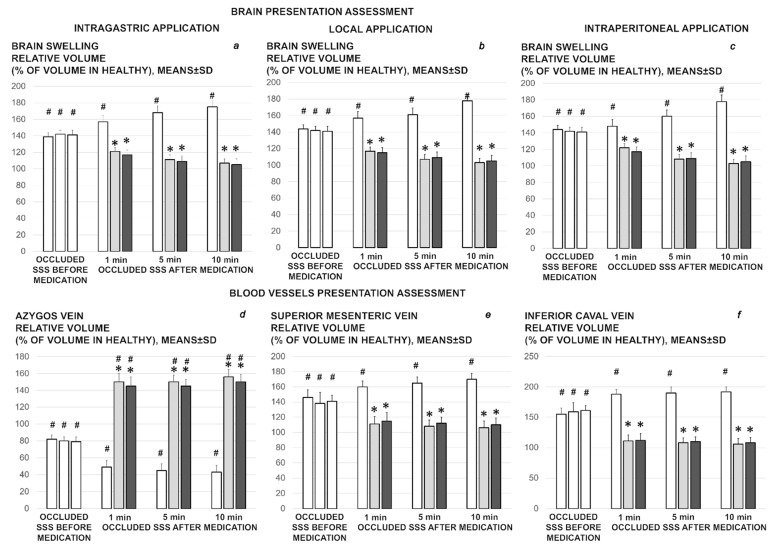
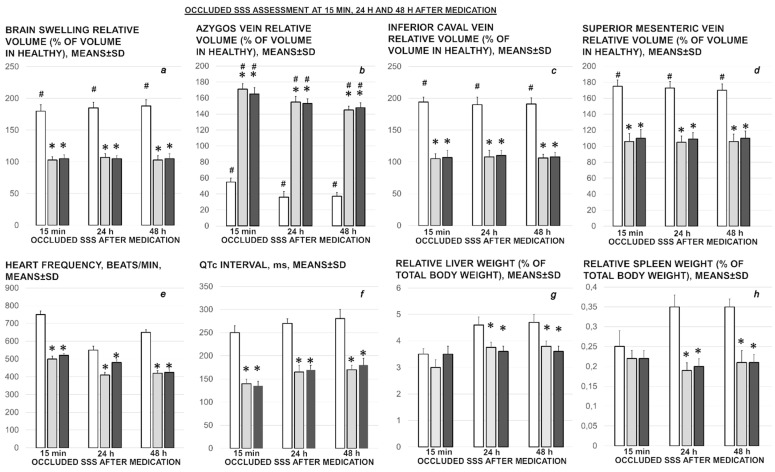
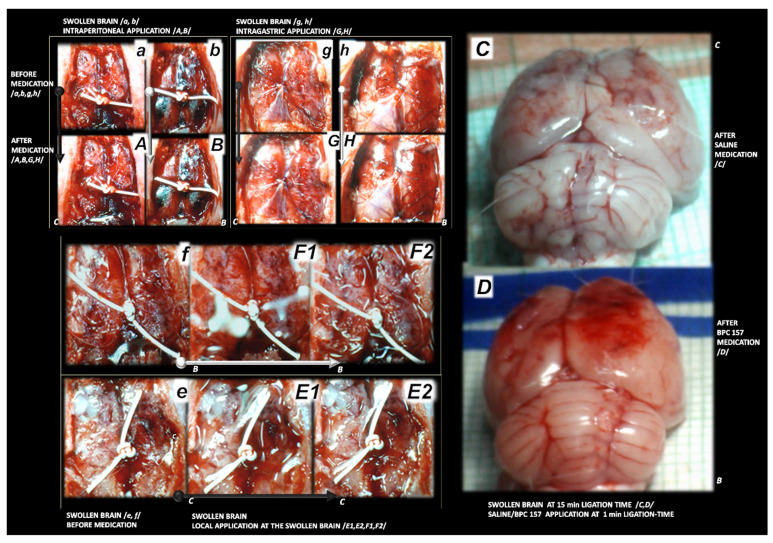
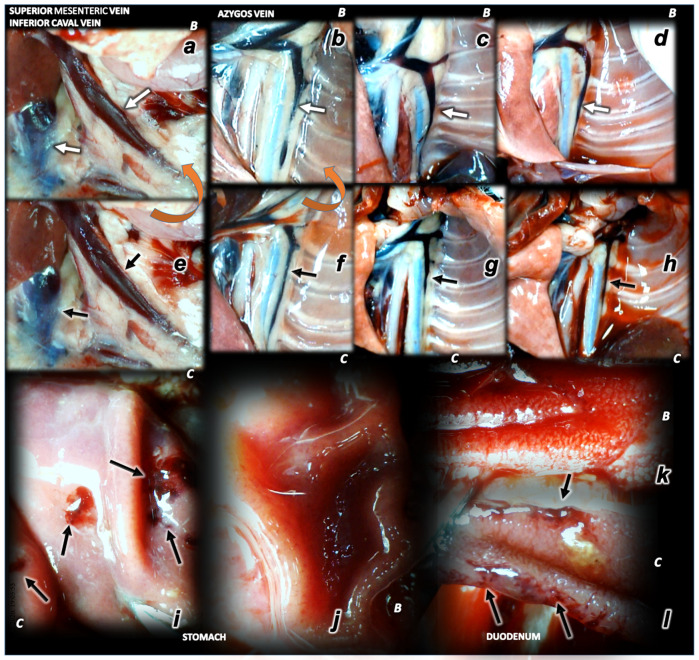
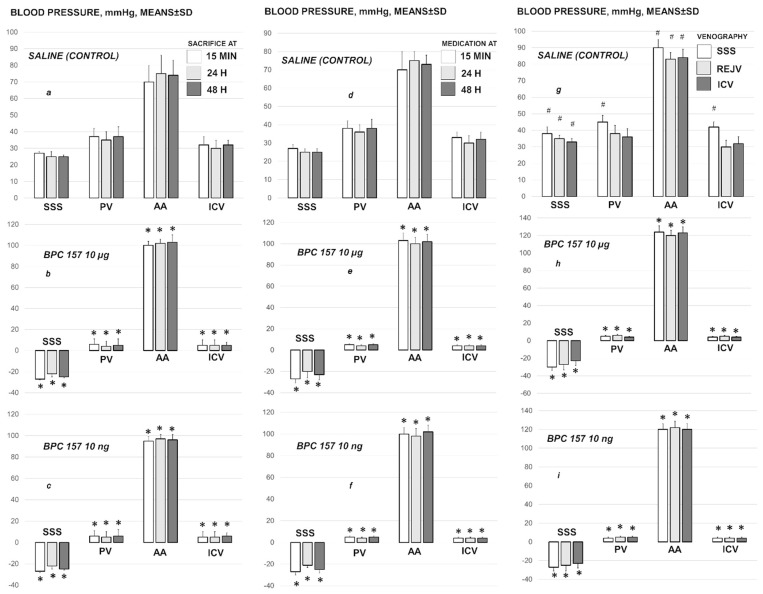
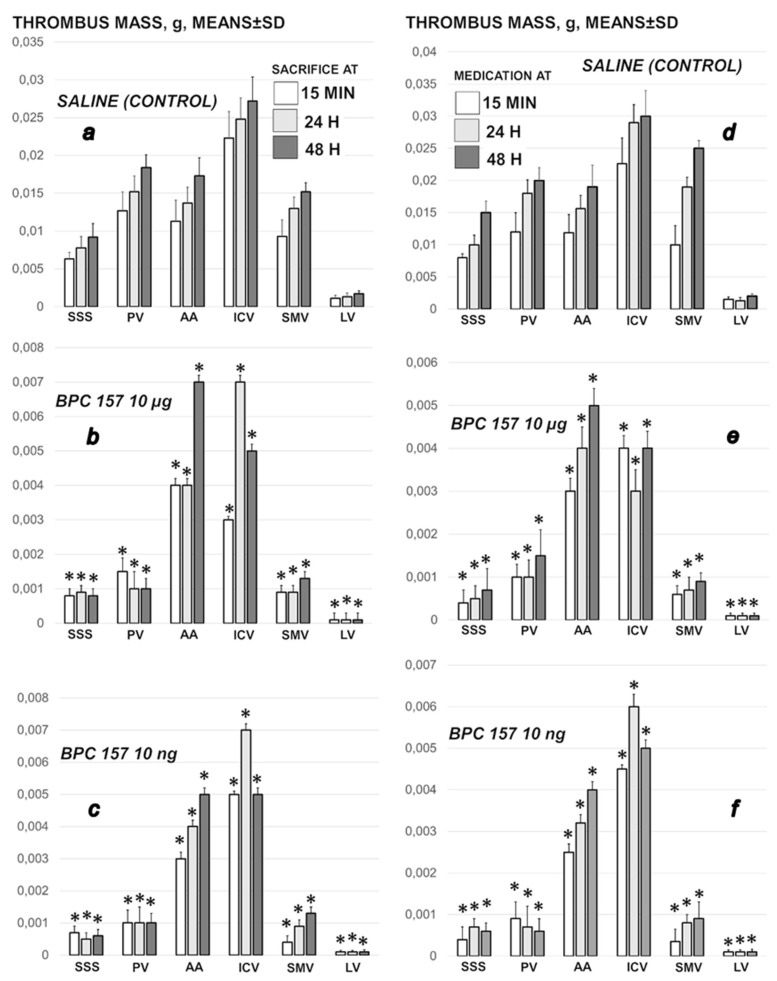
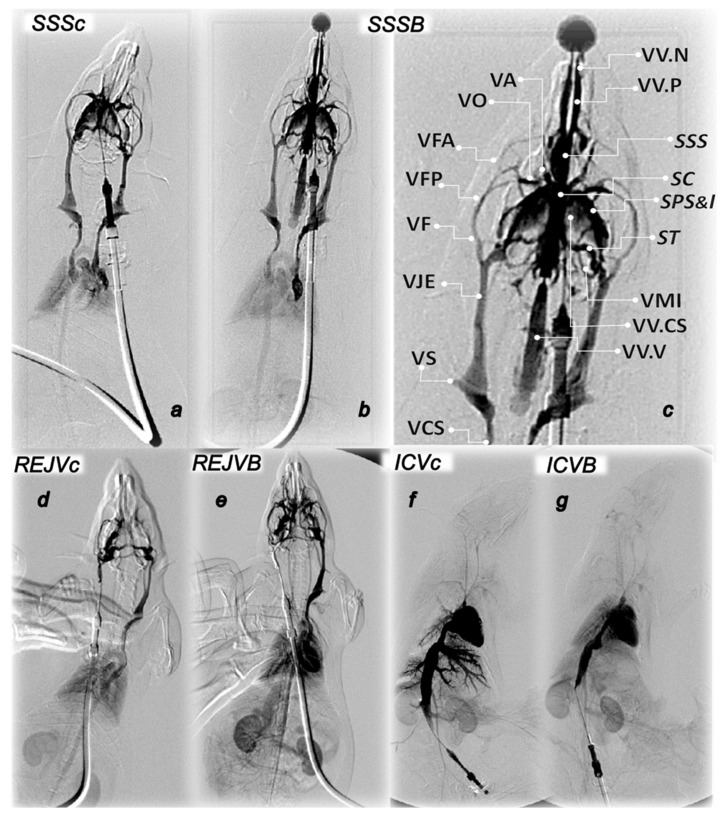
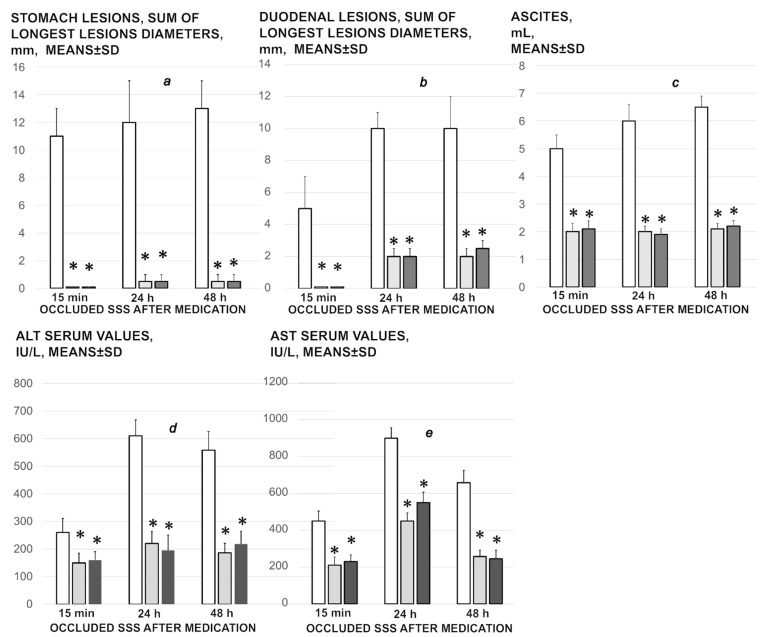
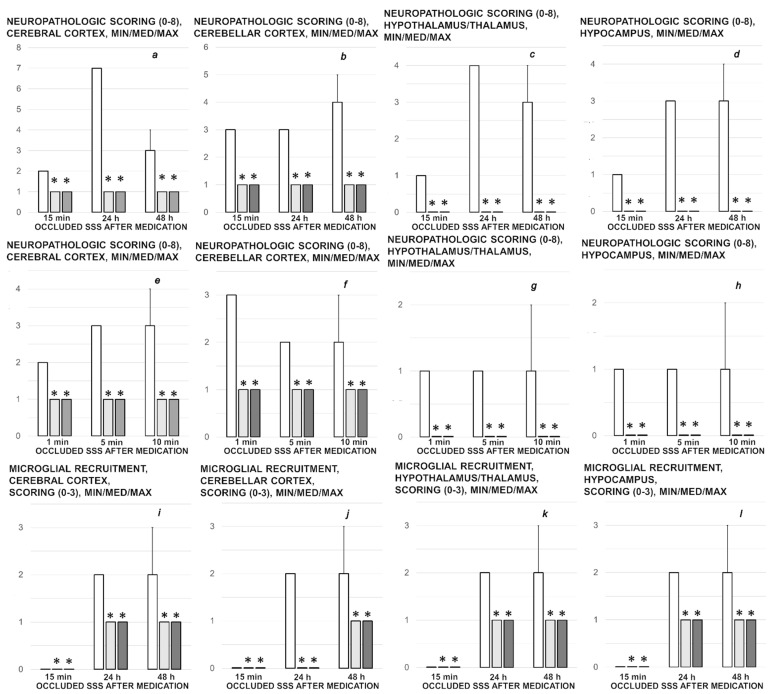
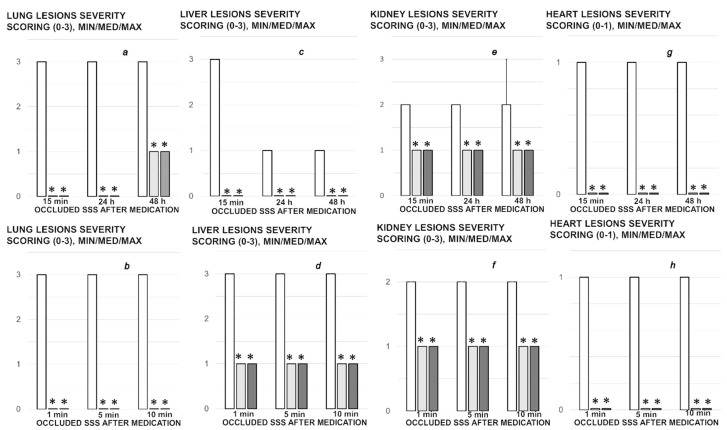
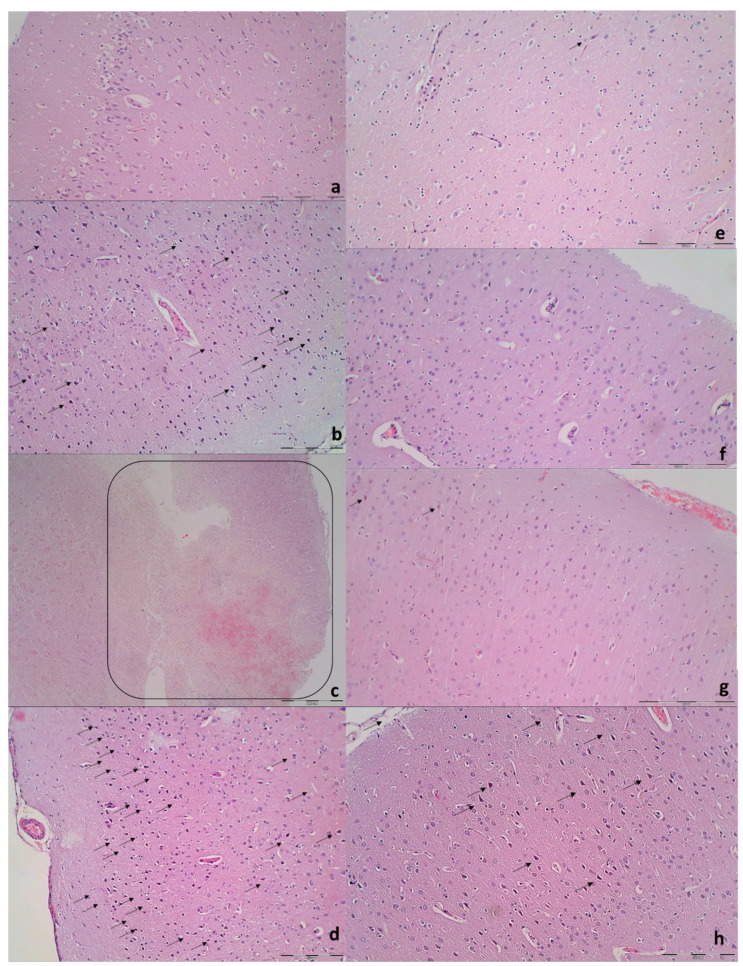
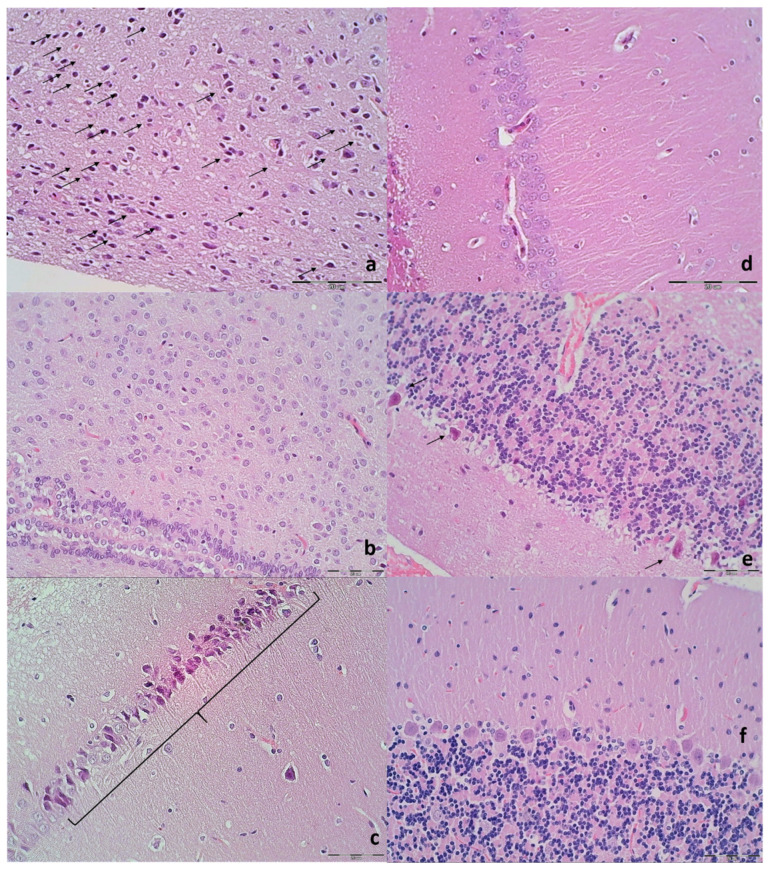
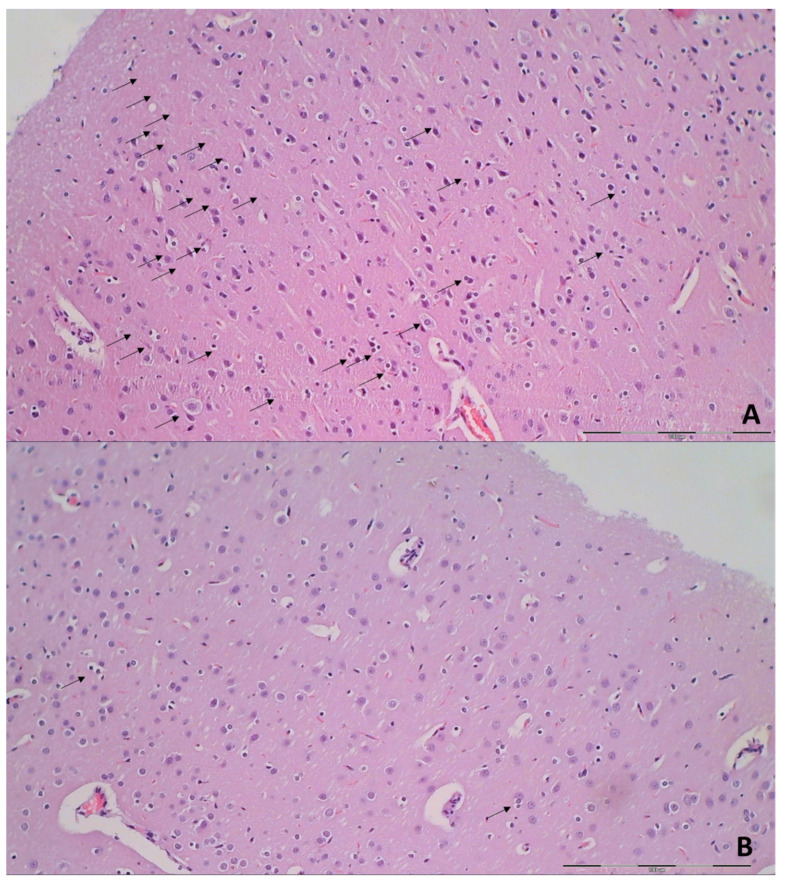
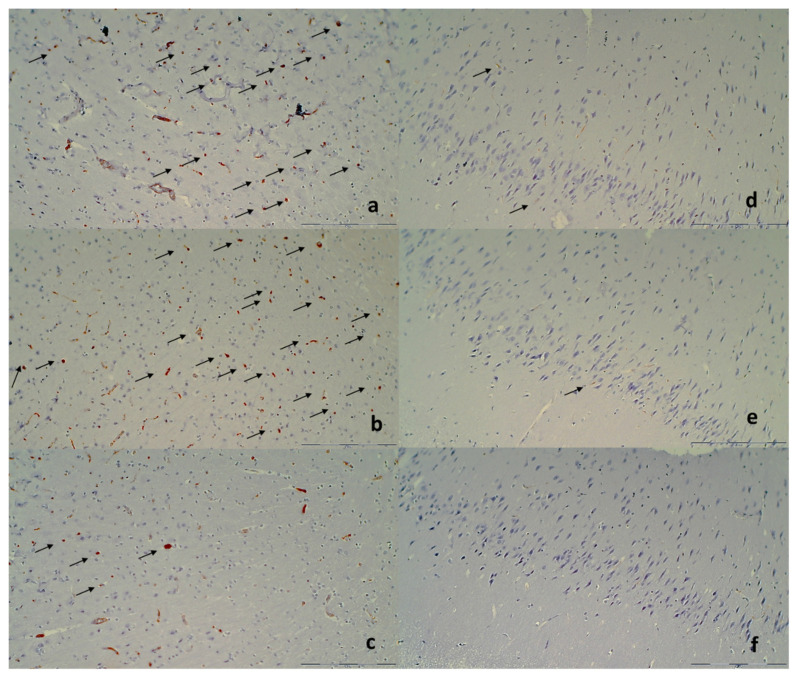
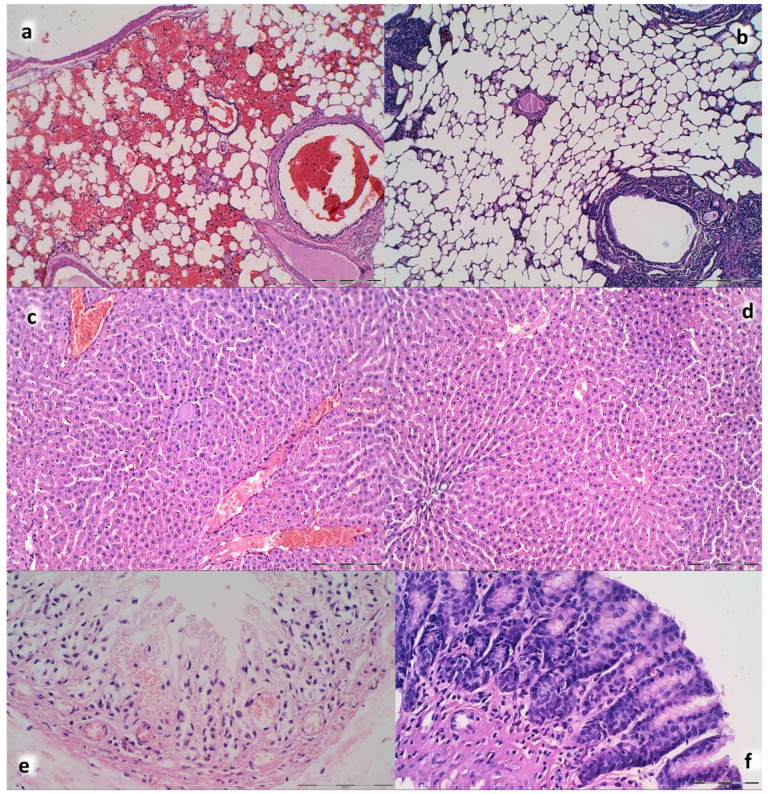
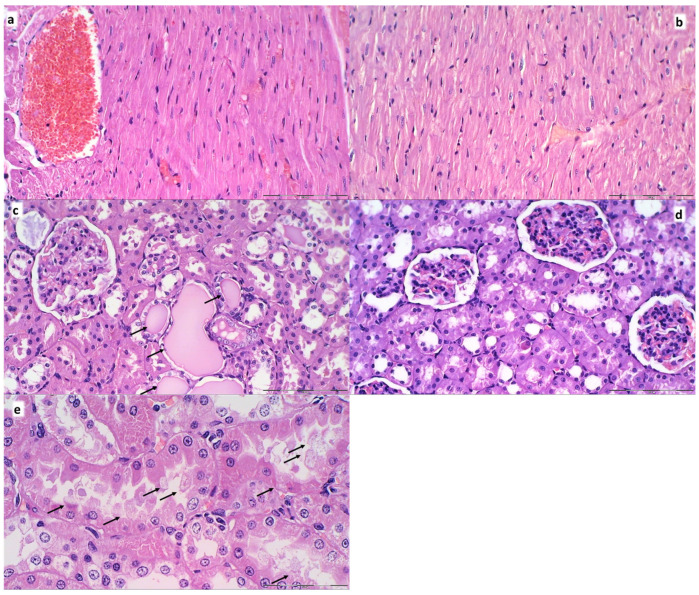
We show the complex syndrome of the occluded superior sagittal sinus, brain swelling and lesions and multiple peripheral organs lesions in rat. Recovery goes centrally and peripherally, with the stable gastric pentadecapeptide BPC 157, which alleviated peripheral vascular occlusion disturbances, rapidly activating alternative bypassing pathways. Assessments were gross recording, venography, ECG, pressure, microscopy, biochemistry. The increased pressure in the superior sagittal sinus, portal and caval hypertension, aortal hypotension, arterial and venous thrombosis, severe brain swelling and lesions (cortex (cerebral, cerebellar), hypothalamus/thalamus, hippocampus), particular veins (azygos, superior mesenteric, inferior caval) dysfunction, heart dysfunction, lung congestion as acute respiratory distress syndrome, kidney disturbances, liver failure, and hemorrhagic lesions in gastrointestinal tract were all assessed. Rats received BPC 157 medication (10 µg/kg, 10 ng/kg) intraperitoneally, intragastrically, or topically to the swollen brain at 1 min ligation-time, or at 15 min, 24 h and 48 h ligation-time. BPC 157 therapy rapidly attenuates the brain swelling, rapidly eliminates the increased pressure in the ligated superior sagittal sinus and the severe portal and caval hypertension and aortal hypotension, and rapidly recruits collateral vessels, centrally ((para)sagittal venous collateral circulation) and peripherally (left superior caval vein azygos vein-inferior caval vein). In conclusion, as shown by all assessments, BPC 157 acts against the permanent occlusion of the superior sagittal sinus and syndrome (i.e., brain, heart, lung, liver, kidney, gastrointestinal lesions, thrombosis), given at 1 min, 15 min, 24 h or 48 h ligation-time. BPC 157 therapy rapidly overwhelms the permanent occlusion of the superior sagittal sinus in rat.
Keywords: BPC 157; occlusion; rats; superior sagittal sinus; therapy; vascular recruitment.
Conflict of interest statement
The authors declare that there are no conflict of interest.
Figures
References
-
- Sikiric P., Seiwerth S., Brcic L., Sever M., Klicek R., Radic B., Drmic D., Ilic S., Kolenc D. Revised Robert’s cytoprotection and adaptive cytoprotection and stable gastric pentadecapeptide BPC 157. Possible significance and implications for novel mediator. Curr. Pharm. Des. 2010;16:1224–1234. doi: 10.2174/138161210790945977. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
