

Accurate Prognosis Prediction of Pancreatic Ductal Adenocarcinoma Using Integrated Clinico-Genomic Data of Endoscopic Ultrasound-Guided Fine Needle Biopsy
- PMID: 34205170
- PMCID: PMC8199936
- DOI: 10.3390/cancers13112791
Accurate Prognosis Prediction of Pancreatic Ductal Adenocarcinoma Using Integrated Clinico-Genomic Data of Endoscopic Ultrasound-Guided Fine Needle Biopsy
Abstract
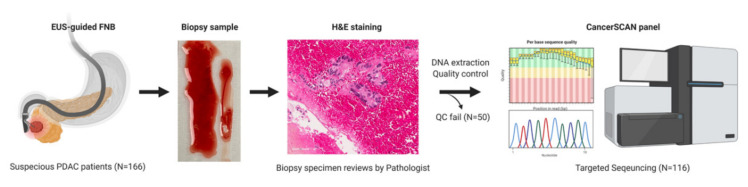
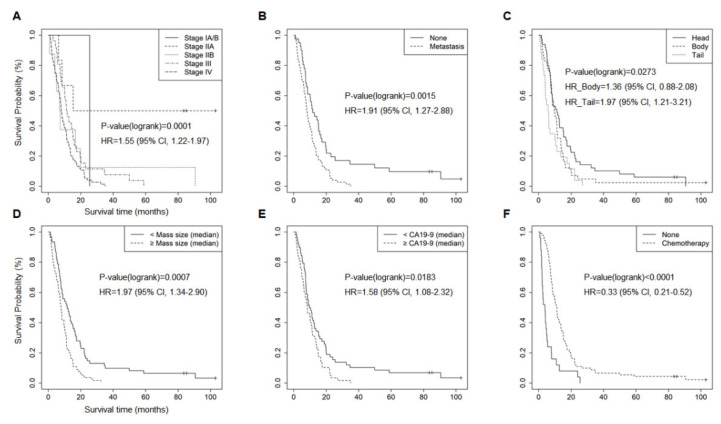
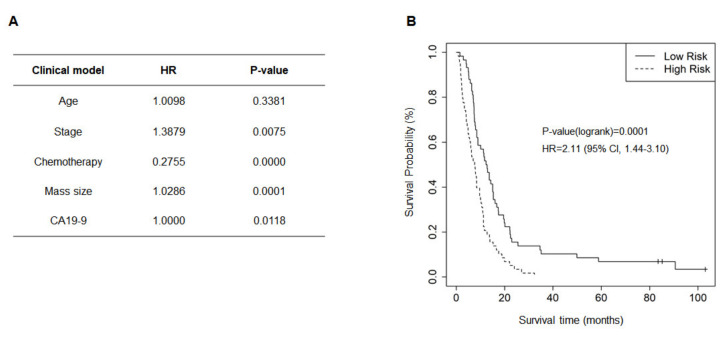
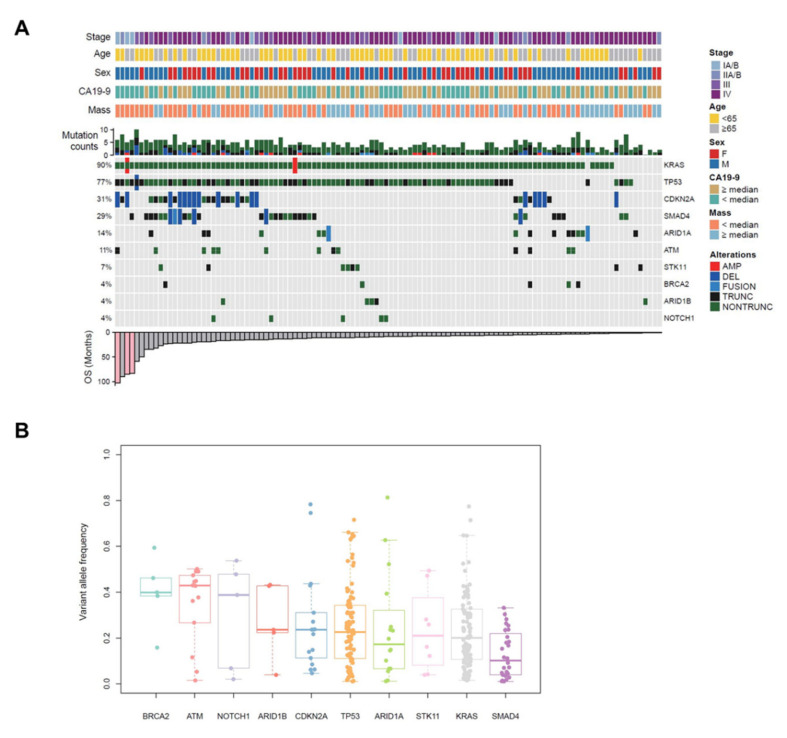
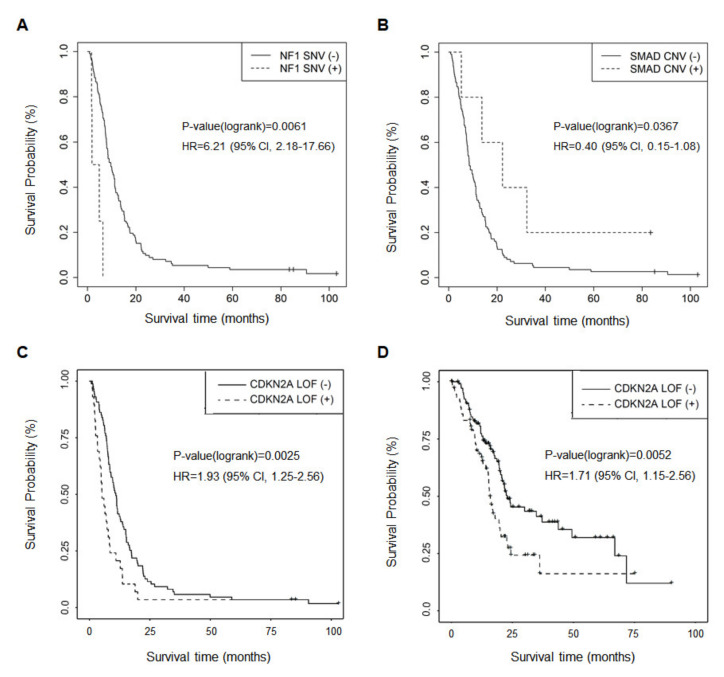
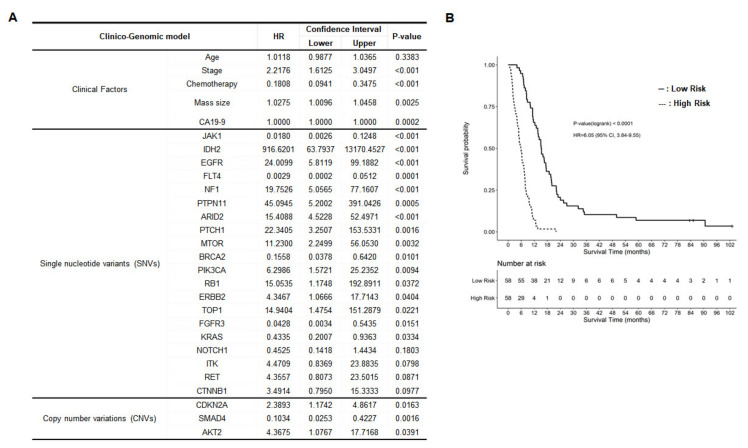
The aim of this study was to investigate the clinical utility of minimal specimens acquired from endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) and perform targeted deep sequencing as a prognosis prediction tool for pancreatic ductal adenocarcinoma (PDAC). A total of 116 specimens with pathologically confirmed PDAC via EUS-FNB were tested using CancerSCAN® panel for a customized targeted deep sequencing. Clinical prognostic factors significantly associated with survival in PDACs were as follows: stage, tumor mass size, tumor location, metastasis, chemotherapy, and initial CA19-9 level. A total of 114 patients (98.3%) had at least a single genetic alteration, and no mutations were detected in two patients, although they were qualified for the targeted deep sequencing. The frequencies of major gene mutations responsible for PDACs were KRAS 90%, CDKN2A 31%, TP53 77%, and SMAD4 29%. A somatic point mutation of NF1, copy number alteration of SMAD4, and loss-of-function of CDKN2A were significantly associated genetic factors for overall survival. Moreover, BRCA2 point mutation was related to liver metastasis. Finally, a clinico-genomic model was developed to estimate the prognosis of patients with PDAC based on clinical parameters and genetic alterations affecting survival in patients; 20 single nucleotide variants and three copy number variations were selected. Targeted deep sequencing on minimal specimens of PDACs was performed, and it was applied to establish a clinico-genomic model for prognosis prediction.
Keywords: clinico-genomic model; endoscopic ultrasound-guided fine needle core biopsy; pancreatic ductal adenocarcinoma; prognosis prediction; targeted deep sequencing.
Conflict of interest statement
There is no conflict to disclose.
Figures
References
-
- Adham M., Jaeck D., Le Borgne J., Oussoultzouglou E., Chenard-Neu M.P., Mosnier J.F., Scoazec J.Y., Mornex F., Partensky C. Long-term survival (5–20 years) after pancreatectomy for pancreatic ductal adenocarcinoma: A series of 30 patients collected from 3 institutions. Pancreas. 2008;37:352–357. doi: 10.1097/MPA.0b013e31818166d2. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
