

Management Challenges of Severe, Complex Dyskinesia. Data from a Large Cohort of Patients Treated with Levodopa-Carbidopa Intestinal Gel for Advanced Parkinson's Disease
- PMID: 34206596
- PMCID: PMC8301838
- DOI: 10.3390/brainsci11070826
Management Challenges of Severe, Complex Dyskinesia. Data from a Large Cohort of Patients Treated with Levodopa-Carbidopa Intestinal Gel for Advanced Parkinson's Disease
Abstract
Background: In the advanced stages of Parkinson's disease (APD), complex forms of dyskinesia may severely impair the patient's quality of life.
Objective: In the present study, we aimed to analyze the evolution under LCIG therapy of the most important motor fluctuations and complex disabling dyskinesias, including diphasic dyskinesia.
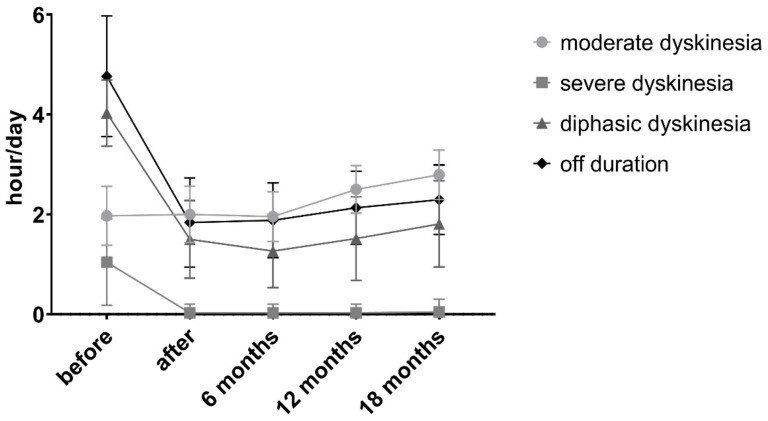
Methods: In this retrospective study, we analyzed the characteristics of patients with APD who had at least 30 min of diphasic dyskinesia (DID) in 3 consecutive days, were considered responders and were treated with LCIG in our clinic. Patients were evaluated before and after PEG and at 6, 12 and 18 months, when the changes in the therapy were recorded, and they completed a 7-point Global Patient Impression of Improvement (PGI-I) scale.
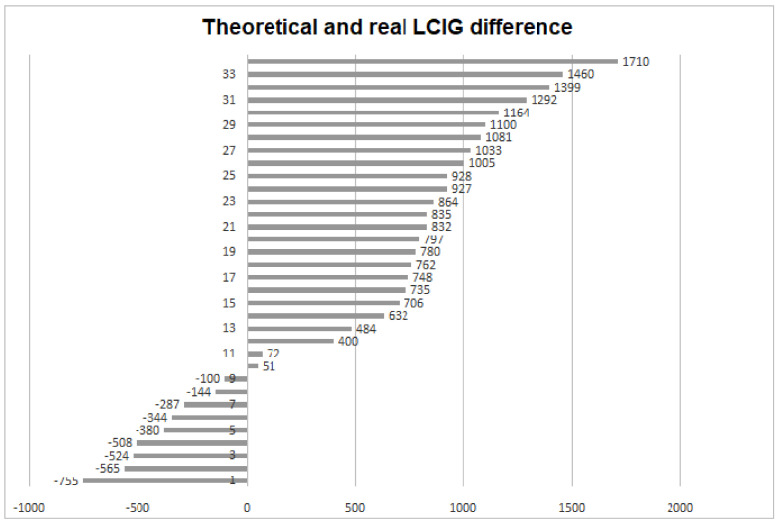
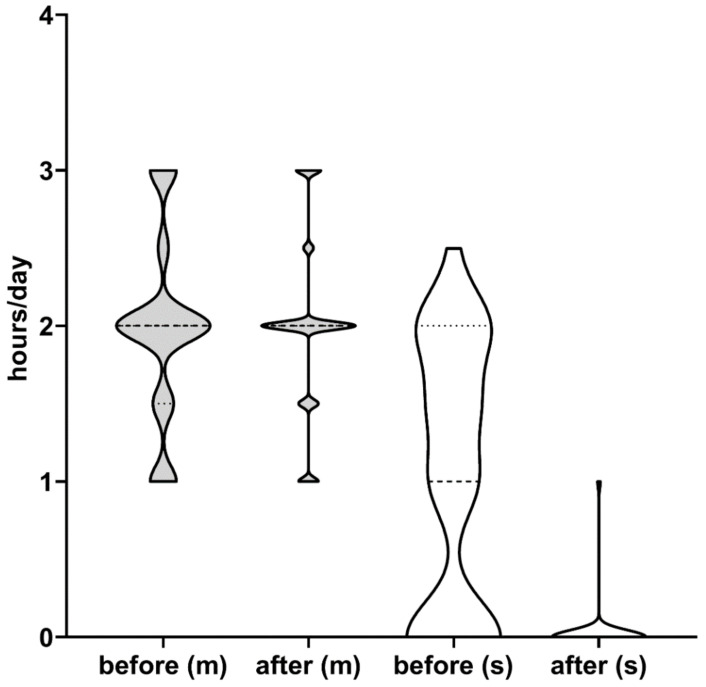
Results: Forty patients fulfilled the inclusion criteria-out of which, 34 performed all visits. There was a substantial difference between the calculated and real LCIG (1232 ± 337 mg vs. 1823 ± 728 mg). The motor fluctuations and most dyskinesias improved significantly after starting LCIG, but an increasing number of patients needed longer daily administrations of LCIG (24 instead of 16 h).
Conclusions: Patients with APD with complex dyskinesias must be tested in dedicated hospitals, and they need a special therapeutic approach. The properly adapted LCIG treatment regarding the dose and time of administration completed with well-selected add-on medication should offer improvement for patients who want to or can only choose this DAT vs. others.
Keywords: advanced Parkinson’s disease; diphasic dyskinesia; levodopa-carbidopa intestinal gel; motor complications.
Conflict of interest statement
S.J.A. consultant and speaking honoraria: AbbVie, Boehringer-Ingelheim, GSK, Lundbeck, Novartis, Pfizer, Teva and UCB. C.V.A. speaking honoraria: AbbVie, Bayer, UCB and Wörwag Pharma. B.L.A. speaking honoraria: AbbVie, Alfasigma, Sanofi. M.C. speaking honoraria AbbVie. Alfasigma, Krka, Naturpharma, SunWave and Terapia SA. M Simu received honoraria for lecturing at symposia and consultancy from AbbVie, AOP Orphan, Boehringer Ingelheim, Krka, Merck, Sanofi, Servier Pharma, Teva and UCB Pharma. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript or in the decision to publish the results.
Figures
References
-
- Ferreira J.J., Katzenschlager R., Bloem B.R., Bonuccelli U., Burn D., Deuschl G., Dietrichs E., Fabbrini G., Friedman A., Kanovsky P., et al. Summary of the recommendations of the EFNS/MDS-ES review on therapeutic management of Parkinson’s disease. Eur. J. Neurol. 2013;20:5–15. doi: 10.1111/j.1468-1331.2012.03866.x. - DOI - PubMed
-
- Odin P., Ray Chaudhuri K., Slevin J.T., Volkmann J., Dietrichs E., Martinez-Martin P., Krauss J.K., Henriksen T., Katzenschlager R., Antonini A., et al. Collective physician perspectives on non-oral medication approaches for the management of clinically relevant unresolved issues in Parkinson’s disease: Consensus from an international survey and discussion program. Park. Relat. Disord. 2015;21:1133–1144. doi: 10.1016/j.parkreldis.2015.07.020. - DOI - PubMed
-
- Olanow C.W., Kieburtz K., Odin P., Espay A.J., Standaert D.G., Fernandez H.H., Vanagunas A., Othman A.A., Widnell K.L., Robieson W.Z., et al. Continuous intrajejunal infusion of levodopa-carbidopa intestinal gel for patients with advanced Parkinson’s disease: A randomised, controlled, double-blind, double-dummy study. Lancet Neurol. 2014;13:141–149. doi: 10.1016/S1474-4422(13)70293-X. - DOI - PMC - PubMed
-
- Antonini A., Poewe W., Chaudhuri K.R., Jech R., Pickut B., Pirtošek Z., Szasz J., Valldeoriola F., Winkler C., Bergmann L., et al. Levodopa-carbidopa intestinal gel in advanced Parkinson’s: Final results of the GLORIA registry. Park. Relat. Disord. 2017;45:13–20. doi: 10.1016/j.parkreldis.2017.09.018. - DOI - PubMed
LinkOut - more resources
Full Text Sources
