

Deep Learning-Based Post-Processing of Real-Time MRI to Assess and Quantify Dynamic Wrist Movement in Health and Disease
- PMID: 34208361
- PMCID: PMC8231139
- DOI: 10.3390/diagnostics11061077
Deep Learning-Based Post-Processing of Real-Time MRI to Assess and Quantify Dynamic Wrist Movement in Health and Disease
Abstract
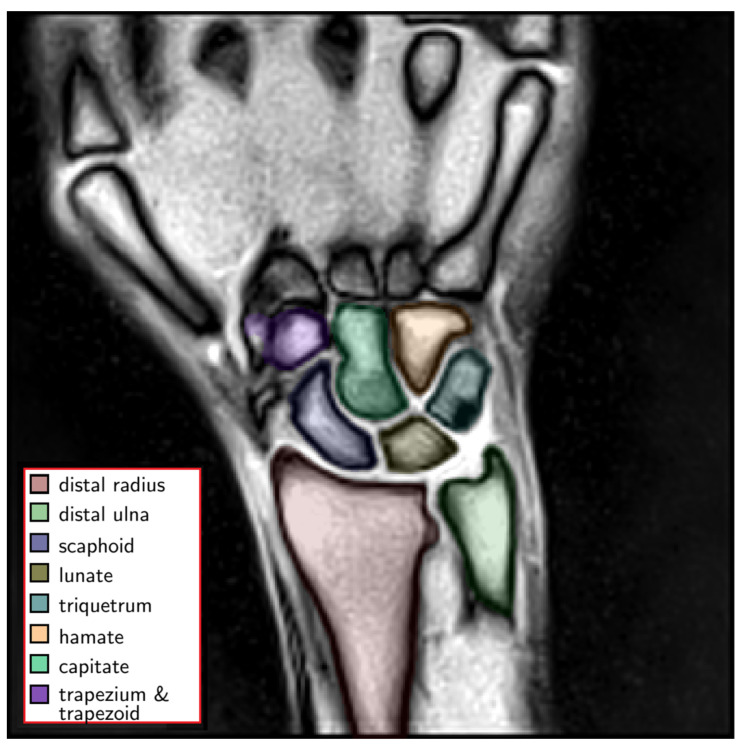
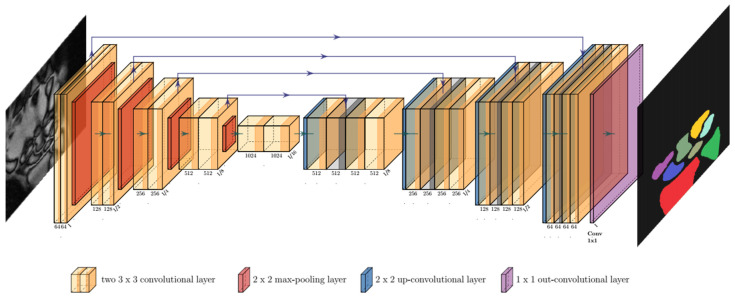
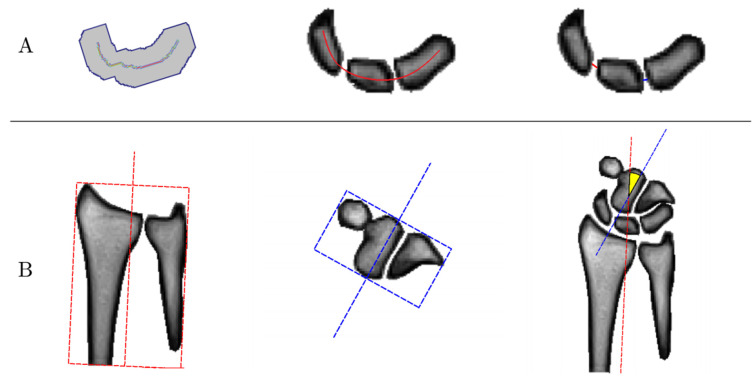
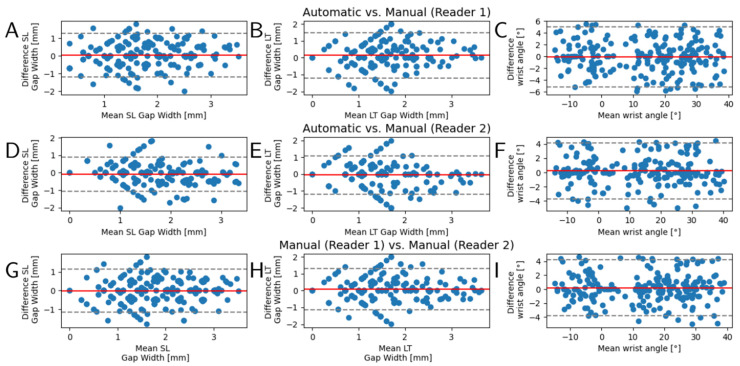
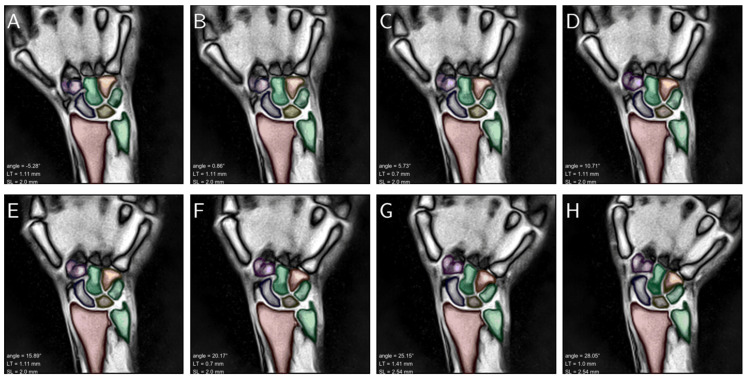
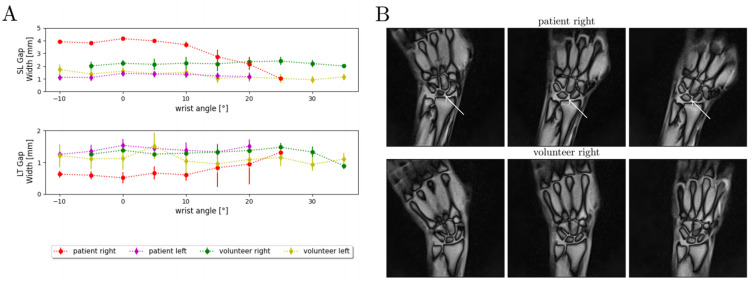
While morphologic magnetic resonance imaging (MRI) is the imaging modality of choice for the evaluation of ligamentous wrist injuries, it is merely static and incapable of diagnosing dynamic wrist instability. Based on real-time MRI and algorithm-based image post-processing in terms of convolutional neural networks (CNNs), this study aims to develop and validate an automatic technique to quantify wrist movement. A total of 56 bilateral wrists (28 healthy volunteers) were imaged during continuous and alternating maximum ulnar and radial abduction. Following CNN-based automatic segmentations of carpal bone contours, scapholunate and lunotriquetral gap widths were quantified based on dedicated algorithms and as a function of wrist position. Automatic segmentations were in excellent agreement with manual reference segmentations performed by two radiologists as indicated by Dice similarity coefficients of 0.96 ± 0.02 and consistent and unskewed Bland-Altman plots. Clinical applicability of the framework was assessed in a patient with diagnosed scapholunate ligament injury. Considerable increases in scapholunate gap widths across the range-of-motion were found. In conclusion, the combination of real-time wrist MRI and the present framework provides a powerful diagnostic tool for dynamic assessment of wrist function and, if confirmed in clinical trials, dynamic carpal instability that may elude static assessment using clinical-standard imaging modalities.
Keywords: carpal instability; deep learning; dynamic instability; magnetic resonance imaging; real-time; scapholunate ligament injury.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyzes, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Theumann N.H., Etechami G., Duvoisin B., Wintermark M., Schnyder P., Favarger N., Gilula L.A. Association between Extrinsic and Intrinsic Carpal Ligament Injuries at MR Arthrography and Carpal Instability at Radiography: Initial Observations. Radiology. 2006;238:950–957. doi: 10.1148/radiol.2383050013. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
