

Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance
- PMID: 34208868
- PMCID: PMC8267838
- DOI: 10.3390/jcm10132932
Transferrin Isoforms, Old but New Biomarkers in Hereditary Fructose Intolerance
Abstract
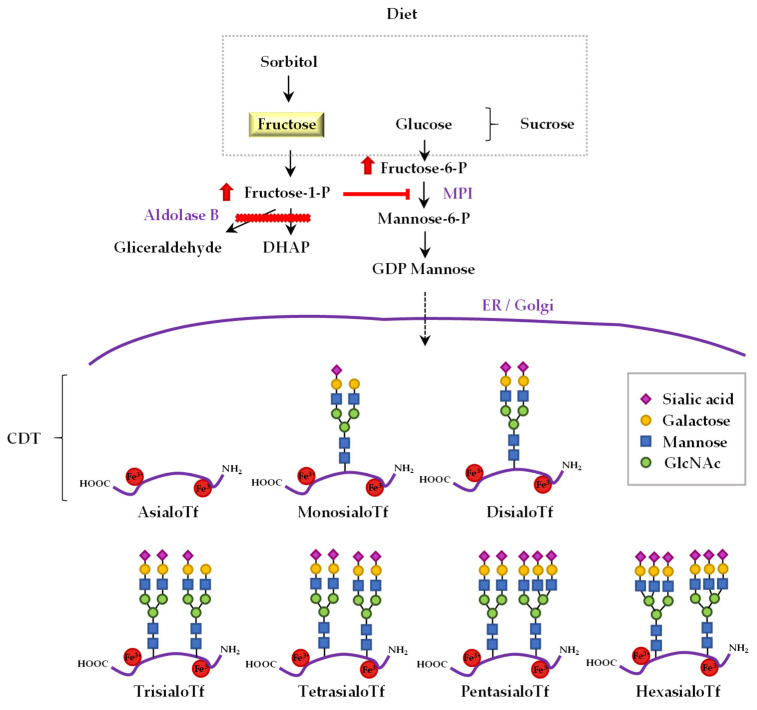
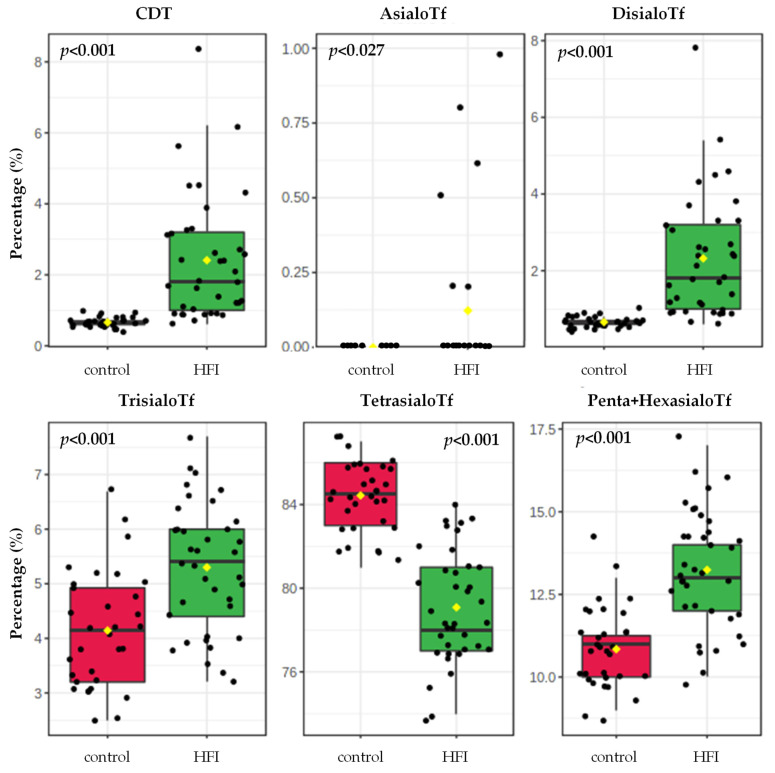
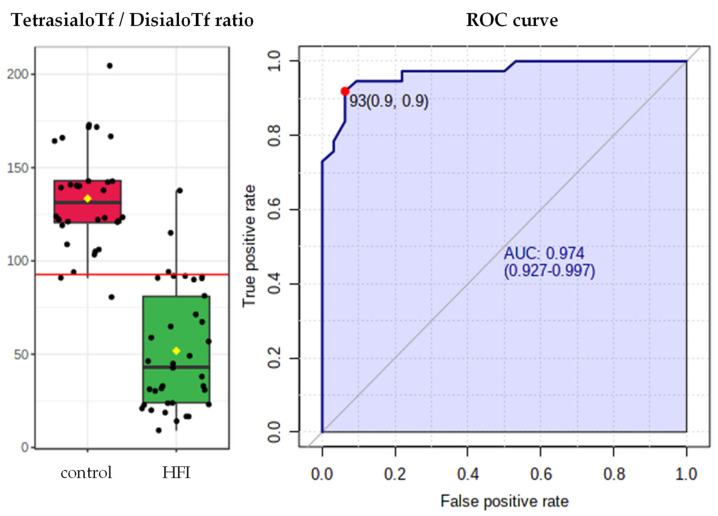
Hereditary Fructose Intolerance (HFI) is an autosomal recessive inborn error of metabolism characterised by the deficiency of the hepatic enzyme aldolase B. Its treatment consists in adopting a fructose-, sucrose-, and sorbitol (FSS)-restrictive diet for life. Untreated HFI patients present an abnormal transferrin (Tf) glycosylation pattern due to the inhibition of mannose-6-phosphate isomerase by fructose-1-phosphate. Hence, elevated serum carbohydrate-deficient Tf (CDT) may allow the prompt detection of HFI. The CDT values improve when an FSS-restrictive diet is followed; however, previous data on CDT and fructose intake correlation are inconsistent. Therefore, we examined the complete serum sialoTf profile and correlated it with FSS dietary intake and with hepatic parameters in a cohort of paediatric and adult fructosemic patients. To do so, the profiles of serum sialoTf from genetically diagnosed HFI patients on an FSS-restricted diet (n = 37) and their age-, sex- and body mass index-paired controls (n = 32) were analysed by capillary zone electrophoresis. We found that in HFI patients, asialoTf correlated with dietary intake of sucrose (R = 0.575, p < 0.001) and FSS (R = 0.475, p = 0.008), and that pentasialoTf+hexasialoTf negatively correlated with dietary intake of fructose (R = -0.386, p = 0.024) and FSS (R = -0.400, p = 0.019). In addition, the tetrasialoTf/disialoTf ratio truthfully differentiated treated HFI patients from healthy controls, with an area under the ROC curve (AUROC) of 0.97, 92% sensitivity, 94% specificity and 93% accuracy.
Keywords: aldolase B; biomarker; diet; fructose; hereditary fructose intolerance; sialotransferrin profile; sorbitol; sucrose.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hereditary Fructose Intolerance—StatPearls—NCBI Bookshelf. [(accessed on 26 December 2020)]; Available online: https://www.ncbi.nlm.nih.gov/books/NBK559102/
-
- Fagerberg L., Hallstrom B.M., Oksvold P., Kampf C., Djureinovic D., Odeberg J., Habuka M., Tahmasebpoor S., Danielsson A., Edlund K., et al. Analysis of the human tissue-specific expression by genome-wide integration of transcriptomics and antibody-based proteomics. Mol. Cell. Proteom. 2014;13:397–406. doi: 10.1074/mcp.M113.035600. - DOI - PMC - PubMed
-
- Santer R., Rischewski J., von Weihe M., Niederhaus M., Schneppenheim S., Baerlocher K., Kohlschütter A., Muntau A., Posselt H.G., Steinmann B., et al. The spectrum of aldolase B (ALDOB) mutations and the prevalence of hereditary fructose intolerance in Central Europe. Hum. Mutat. 2005;25:594. doi: 10.1002/humu.9343. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
