

Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study
- PMID: 34209578
- PMCID: PMC8269374
- DOI: 10.3390/cancers13133244
Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study
Abstract
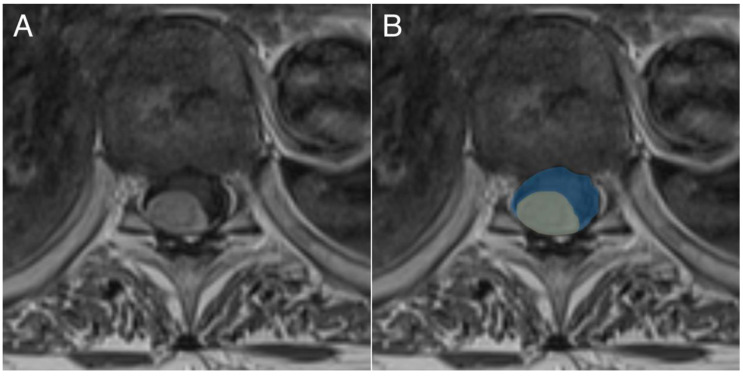
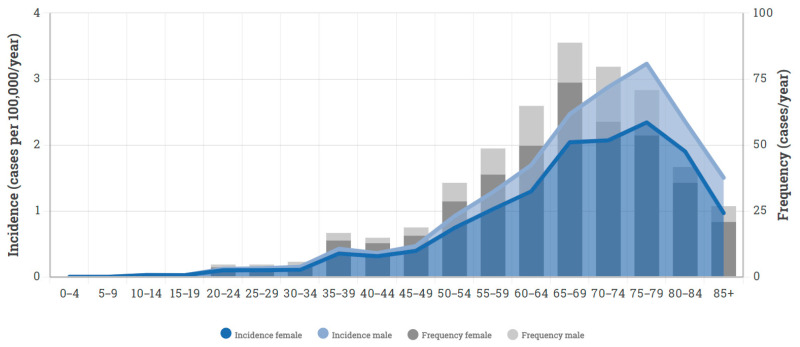
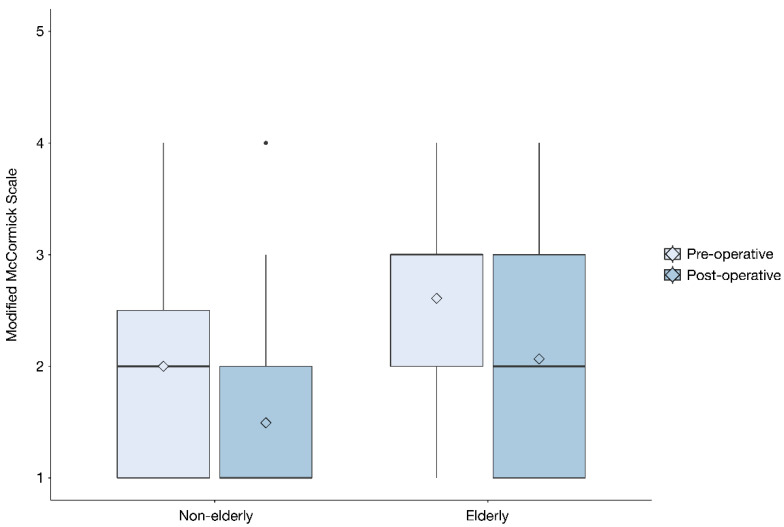
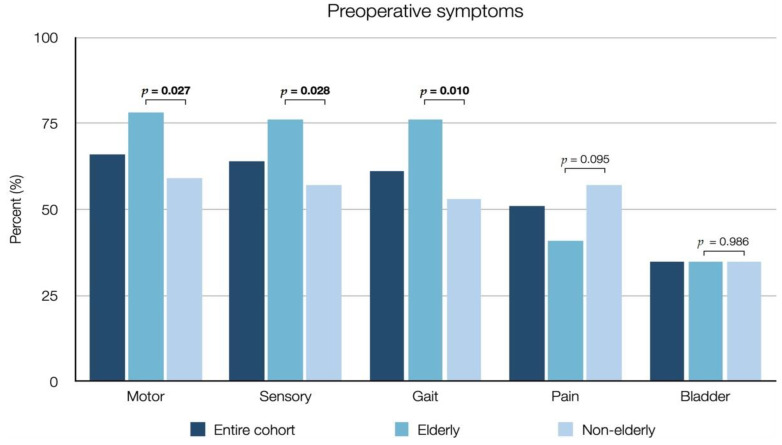
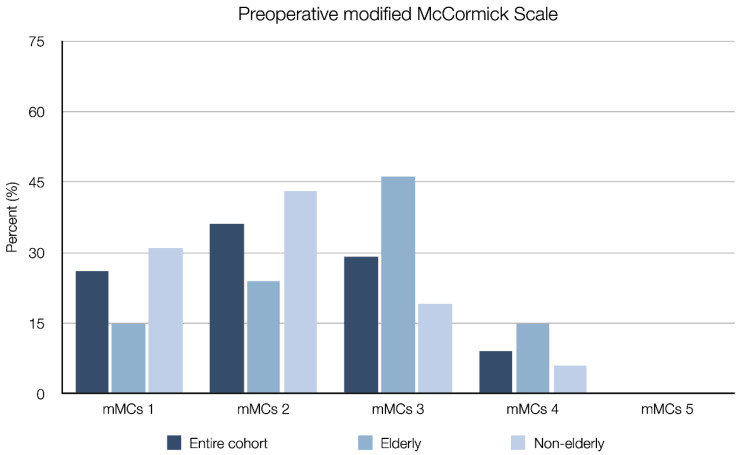
Spinal meningiomas are the most common adult primary spinal tumor, constituting 24-45% of spinal intradural tumors and 2% of all meningiomas. The aim of this study was to assess postoperative complications, long-term outcomes, predictors of functional improvement and differences between elderly (≥70 years) and non-elderly (18-69 years) patients surgically treated for spinal meningiomas. Variables were retrospectively collected from patient charts and magnetic resonance images. Baseline comparisons, paired testing and regression analyses were used. In conclusion, 129 patients were included, with a median follow-up time of 8.2 years. Motor deficit was the most common presenting symptom (66%). The median time between diagnosis and surgery was 1.3 months. A postoperative complication occurred in 10 (7.8%) and tumor growth or recurrence in 6 (4.7%) patients. Surgery was associated with significant improvement of motor and sensory deficit, gait disturbance, bladder dysfunction and pain. Time to surgery, tumor area and the degree of spinal cord compression significantly predicted postoperative improvement in a modified McCormick scale (mMCs) in the univariable regression analysis, and spinal cord compression showed independent risk association in multivariable analysis. There was no difference in improvement, complications or tumor control between elderly and non-elderly patients. We concluded that surgery of spinal meningiomas was associated with significant long-term neurological improvement, which could be predicted by time to surgery, tumor size and spinal cord compression.
Keywords: age; elderly; meningioma; neurosurgery; spinal meningioma; spine; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Yamaguchi S., Menezes A.H., Shimizu K., Woodroffe R.W., Helland L.C., Hitchon P.W., Howard M.A. Differences and characteristics of symptoms by tumor location, size, and degree of spinal cord compression: A retrospective study on 53 surgically treated, symptomatic spinal meningiomas. J. Neurosurg. Spine. 2020;32:931–940. doi: 10.3171/2019.12.SPINE191237. - DOI - PubMed
LinkOut - more resources
Full Text Sources
