

Supplemental Association of Clonal Hematopoiesis With Incident Heart Failure
- PMID: 34210413
- PMCID: PMC8313294
- DOI: 10.1016/j.jacc.2021.04.085
Supplemental Association of Clonal Hematopoiesis With Incident Heart Failure
Erratum in
-
Correction.J Am Coll Cardiol. 2021 Aug 17;78(7):762. doi: 10.1016/j.jacc.2021.06.032. J Am Coll Cardiol. 2021. PMID: 34384560 No abstract available.
Abstract
Background: Age-related clonal hematopoiesis of indeterminate potential (CHIP), defined as clonally expanded leukemogenic sequence variations (particularly in DNMT3A, TET2, ASXL1, and JAK2) in asymptomatic individuals, is associated with cardiovascular events, including recurrent heart failure (HF).
Objectives: This study sought to evaluate whether CHIP is associated with incident HF.
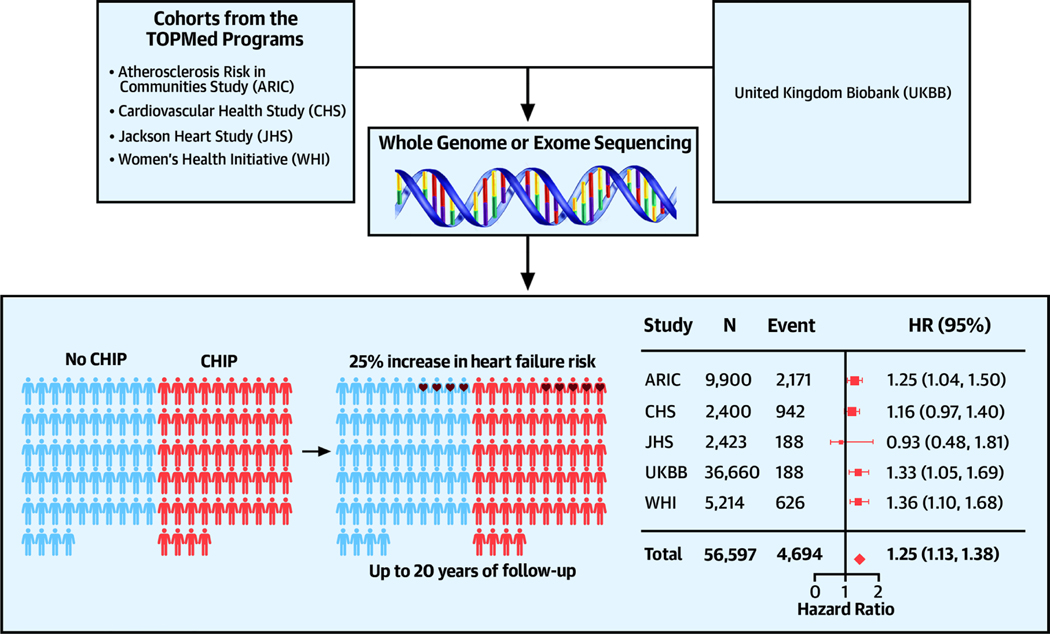
Methods: CHIP status was obtained from whole exome or genome sequencing of blood DNA in participants without prevalent HF or hematological malignancy from 5 cohorts. Cox proportional hazards models were performed within each cohort, adjusting for demographic and clinical risk factors, followed by fixed-effect meta-analyses. Large CHIP clones (defined as variant allele frequency >10%), HF with or without baseline coronary heart disease, and left ventricular ejection fraction were evaluated in secondary analyses.
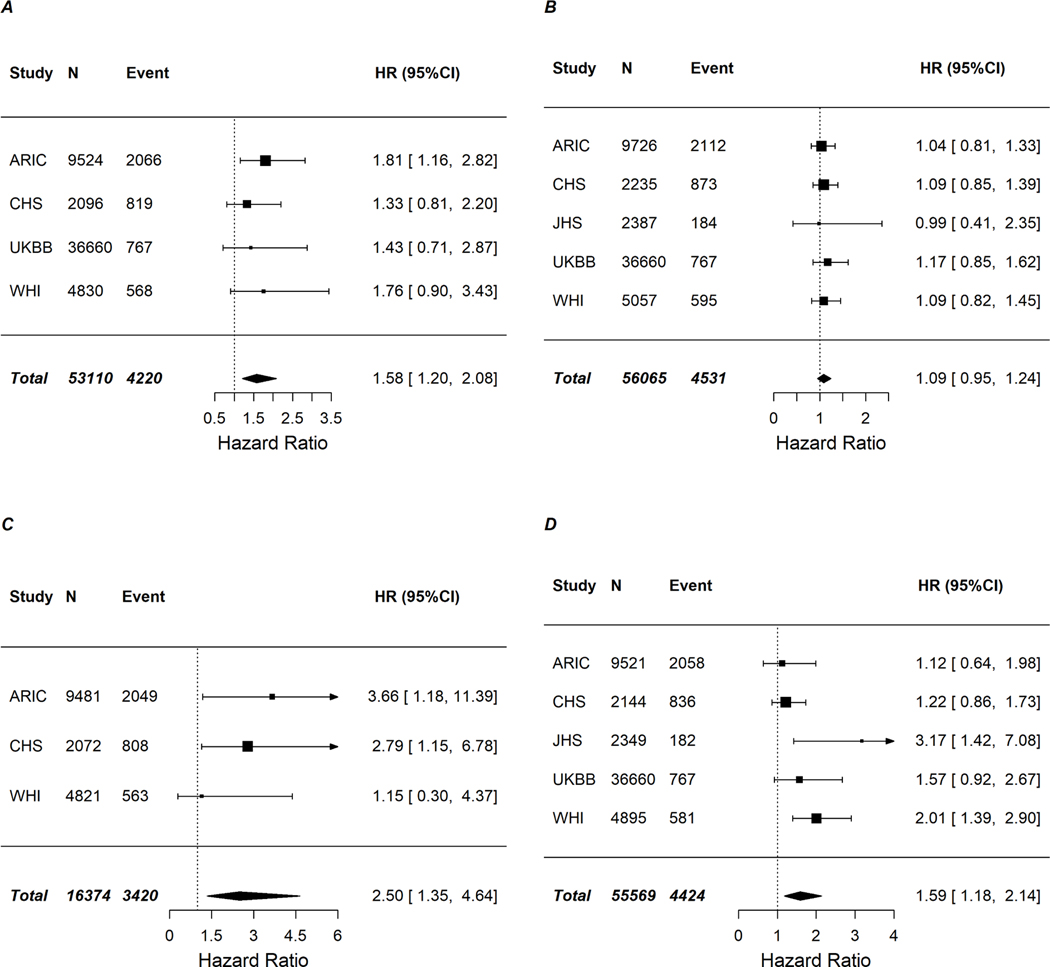
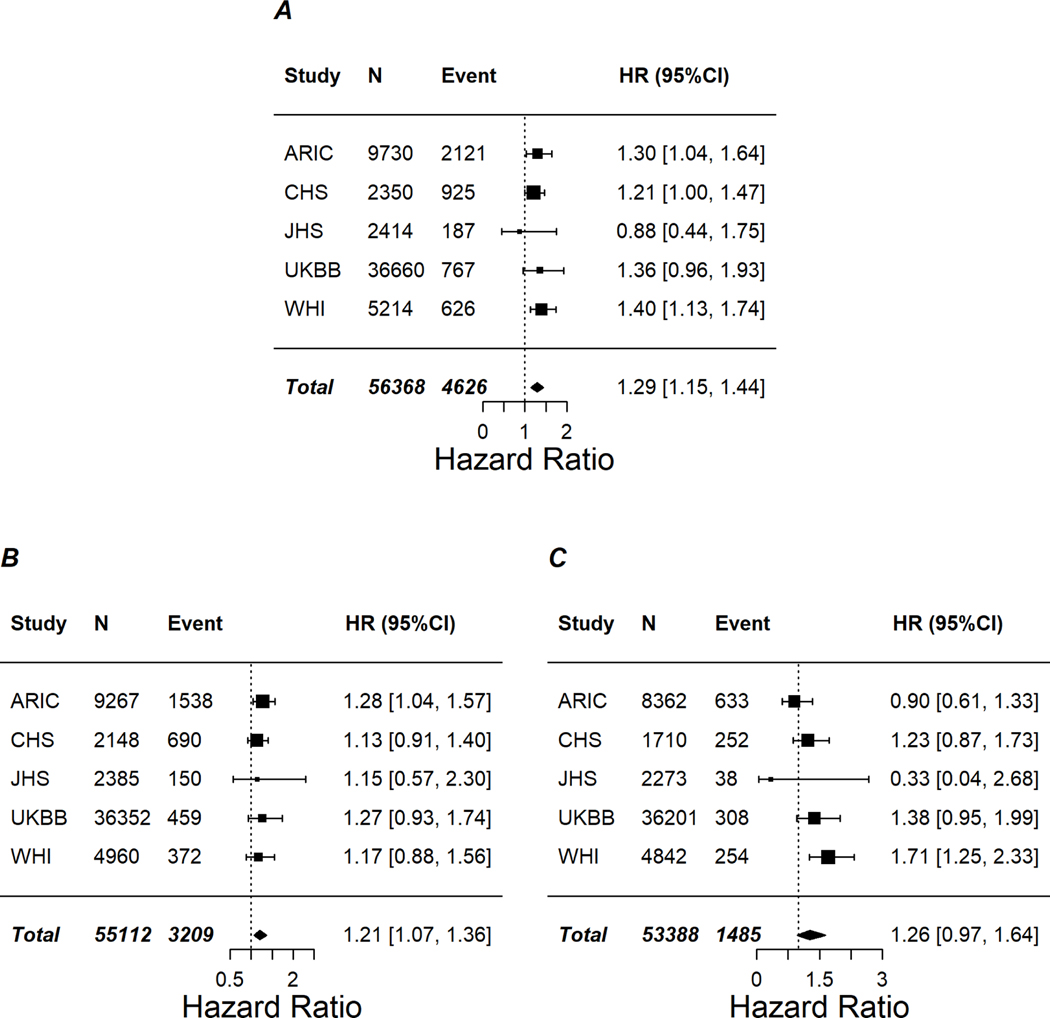
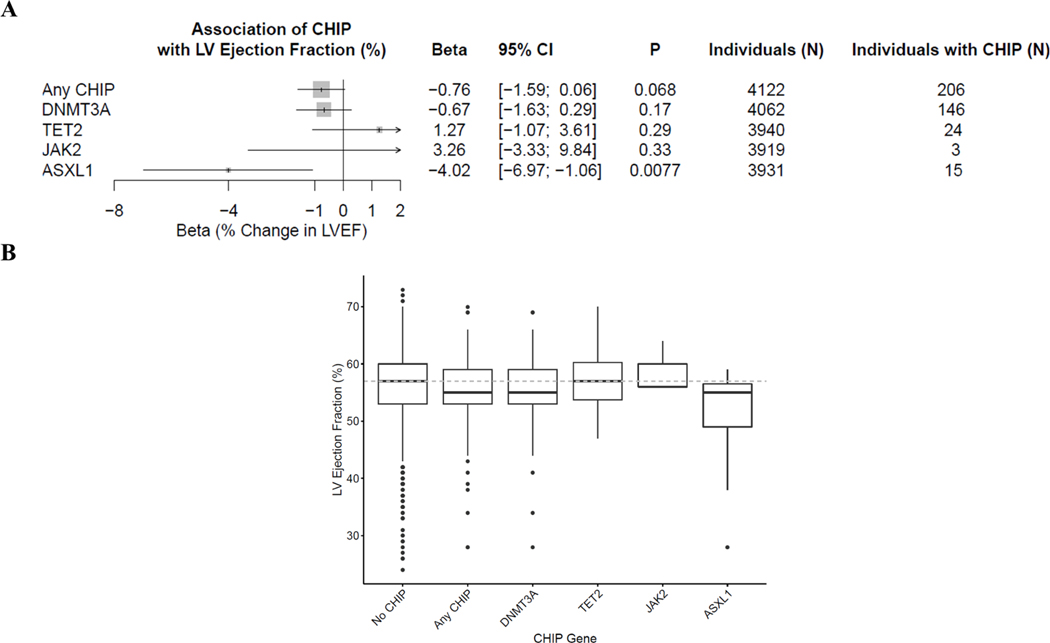
Results: Of 56,597 individuals (59% women, mean age 58 years at baseline), 3,406 (6%) had CHIP, and 4,694 developed HF (8.3%) over up to 20 years of follow-up. CHIP was prospectively associated with a 25% increased risk of HF in meta-analysis (hazard ratio: 1.25; 95% confidence interval: 1.13-1.38) with consistent associations across cohorts. ASXL1, TET2, and JAK2 sequence variations were each associated with an increased risk of HF, whereas DNMT3A sequence variations were not associated with HF. Secondary analyses suggested large CHIP was associated with a greater risk of HF (hazard ratio: 1.29; 95% confidence interval: 1.15-1.44), and the associations for CHIP on HF with and without prior coronary heart disease were homogenous. ASXL1 sequence variations were associated with reduced left ventricular ejection fraction.
Conclusions: CHIP, particularly sequence variations in ASXL1, TET2, and JAK2, represents a new risk factor for HF.
Keywords: clonal hematopoiesis of indeterminate potential; heart failure; risk factor.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Whole genome sequencing (WGS) for the Trans-Omics in Precision Medicine (TOPMed) program was supported by the National Heart, Lung, and Blood Institute (NHLBI). WGS for “NHLBI TOPMed: The Jackson Heart Study” (phs000964) was performed at the University of Washington Northwest Genomics Center (HHSN268201100037C). WGS for “NHLBI TOPMed: Women's Health Initiative (WHI)” (phs001237) was performed at the Broad Institute (HHSN268201500014C). WGS for “NHLBI TOPMed: Trans-Omics for Precision Medicine (TOPMed) Whole Genome Sequencing Project: Cardiovascular Health Study” (phs001368) was performed at Baylor (HHSN268201600033I, 3U54HG003273-12S2/HHSN268201500015C). Centralized read mapping and genotype calling along with variant quality metrics and filtering were provided by the TOPMed Informatics Research Center (3R01HL-117626-02S1; contract HHSN268201800002I). Phenotype harmonization, data management, sample-identity QC, and general study coordination were provided by the TOPMed Data Coordinating Center (3R01HL-120393-02S1; contract HHSN268201800001I). The Atherosclerosis Risk In Communities study has been funded in whole or in part with federal funds from the NHLBI, National Institutes of Health, Department of Health and Human Services (contract numbers HHSN268201700001I, HHSN268201700002I, HHSN268201700003I, HHSN268201700004I, and HHSN268201700005I). Funding support for “Building on GWAS for NHLBI-diseases: the U.S. CHARGE consortium” was provided by the National Institutes of Health through the American Recovery and Reinvestment Act of 2009 (5RC2HL102419). Whole exome sequencing was carried out at the Baylor College of Medicine Human Genome Sequencing Center (U54 HG003273 and R01HL086694). The CHS (Cardiovascular Health Study) was supported by contracts HHSN268201200036C, HHSN268200800007C, HHSN268201800001C, N01HC55222, N01HC85079, N01HC85080, N01HC85081, N01HC85082, N01HC85083, N01HC85086, and 75N92021D00006, and by grants U01HL080295 and U01HL130114 from the NHLBI, with additional contribution from the National Institute of Neurological Disorders and Stroke. Additional support was provided by R01AG023629 from the National Institute on Aging. The JHS (Jackson Heart Study) is supported and conducted in collaboration with Jackson State University (HHSN268201800013I), Tougaloo College (HHSN268201800014I), the Mississippi State Department of Health (HHSN268201800015I), and the University of Mississippi Medical Center (HHSN268201800010I, HHSN268201800011I, and HHSN268201800012I) contracts from the NHLBI and the National Institute on Minority Health and Health Disparities. The WHI program is funded by the NHLBI, National Institutes of Health, U.S. Department of Health and Human Services through contracts HHSN268201600018C, HHSN268201600001C, HHSN268201600002C, HHSN268201600003C, and HHSN268201600004C. Dr Yu is supported in part by R01HL141824 and R01HL148050. Dr Raffield was funded by T32 HL129982 and KL2TR00249. Dr Zekavat is supported by the National Institutes of Health’s NHLBI under award number 1F30HL149180-01 and the National Institutes of Health’s Medical Scientist Training Program at the Yale School of Medicine. Dr Shah is supported in part by grants from the NHLBI (R01HL135008, R01HL143224, R01HL150342, R01HL14818, and K24HL152008); has received research support from Novartis and Philips Ultrasound through Brigham and Women's Hospital; and has received consulting fees from Philips Ultrasound and Edwards Lifesciences. Dr Honigberg is supported by a grant from the NHLBI (T32HL094301-07). Dr Ebert has received research funding from Celgene, Deerfield, and Novartis; has received consulting fees from GRAIL; and has served on the scientific advisory boards and holds equity in Skyhawk Therapeutics, Exo Therapeutics, and Neomorph Therapeutics. Dr Reiner is supported by R01HL148565. Dr Natarajan is supported by grants from the NHLBI (R01HL142711, R01HL148050, R01HL148565) and Fondation Leducq (TNE-18CVD04); has received grants from Amgen, Apple, Boston Scientific, and Novartis; has received consulting income from Apple, Blackstone Life Sciences, Novartis, and Genentech; and has spousal employment at Vertex, all unrelated to the present work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Clonal Hematopoiesis and Incident Heart Failure Risk: The Clone Wars Reach the Myocardium.J Am Coll Cardiol. 2021 Jul 6;78(1):53-55. doi: 10.1016/j.jacc.2021.04.084. J Am Coll Cardiol. 2021. PMID: 34210414 No abstract available.
References
-
- Stewart S, Ekman I, Ekman T, Oden A, Rosengren A. Population impact of heart failure and the most common forms of cancer: a study of 1 162 309 hospital cases in Sweden (1988 to 2004). Circ Cardiovasc Qual Outcomes 2010;3:573–80. - PubMed
-
- Ayachi S, Buscarlet M, Busque L. 60 Years of clonal hematopoiesis research: From X-chromosome inactivation studies to the identification of driver mutations. Exp Hematol 2020;83:2–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201800012C/HL/NHLBI NIH HHS/United States
- R01 HL120393/HL/NHLBI NIH HHS/United States
- HHSN268201600002C/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- R01 HL148565/HL/NHLBI NIH HHS/United States
- R01 HL086694/HL/NHLBI NIH HHS/United States
- U54 HG003273/HG/NHGRI NIH HHS/United States
- HHSN268201800014C/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201800012I/HL/NHLBI NIH HHS/United States
- HHSN268201800011C/HL/NHLBI NIH HHS/United States
- HHSN268201800015I/HB/NHLBI NIH HHS/United States
- HHSN268201800011I/HB/NHLBI NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- HHSN268201100037C/HL/NHLBI NIH HHS/United States
- T32 HL094301/HL/NHLBI NIH HHS/United States
- RC2 HL102419/HL/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- F30 HL149180/HL/NHLBI NIH HHS/United States
- R01 HL151283/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- HHSN268201600018C/HL/NHLBI NIH HHS/United States
- HHSN268201800014I/HB/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- T32 HL129982/HL/NHLBI NIH HHS/United States
- R01 HL142711/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- HHSN268201800013I/MD/NIMHD NIH HHS/United States
- HHSN268201500015C/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- HHSN268201600003C/HL/NHLBI NIH HHS/United States
- HHSN268201600033C/ES/NIEHS NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- K24 HL152008/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- HHSN268201600004C/HL/NHLBI NIH HHS/United States
- HHSN268201500014C/HL/NHLBI NIH HHS/United States
- HHSN268201600001C/HL/NHLBI NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- R01 HL141824/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201800010I/HB/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- R01 HL117626/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- R01 HL148050/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
