

Cardiopulmonary exercise capacity and limitations 3 months after COVID-19 hospitalisation
- PMID: 34210791
- PMCID: PMC8247555
- DOI: 10.1183/13993003.00996-2021
Cardiopulmonary exercise capacity and limitations 3 months after COVID-19 hospitalisation
Abstract
Background: This study aimed to describe cardiopulmonary function during exercise 3 months after hospital discharge for COVID-19 and compare groups according to dyspnoea and intensive care unit (ICU) stay.
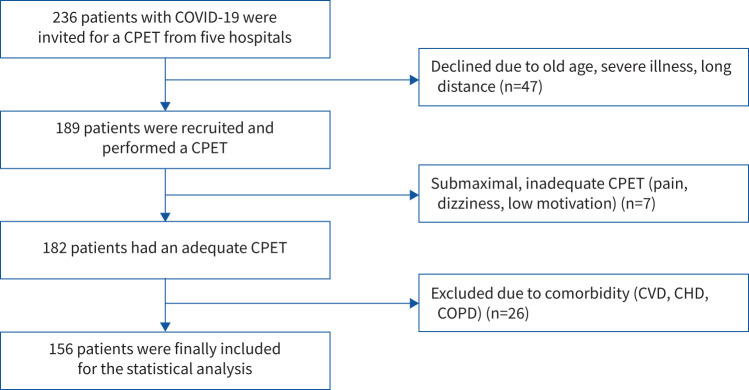
Methods: Participants with COVID-19 discharged from five large Norwegian hospitals were consecutively invited to a multicentre, prospective cohort study. In total, 156 participants (mean age 56.2 years, 60 females) were examined with a cardiopulmonary exercise test (CPET) 3 months after discharge and compared with a reference population. Dyspnoea was assessed using the modified Medical Research Council (mMRC) dyspnoea scale.
Results: Peak oxygen uptake (V'O2 peak) <80% predicted was observed in 31% (n=49). Ventilatory efficiency was reduced in 15% (n=24), while breathing reserve <15% was observed in 16% (n=25). Oxygen pulse <80% predicted was found in 18% (n=28). Dyspnoea (mMRC ≥1) was reported by 47% (n=59). These participants had similar V'O2 peak (p=0.10) but lower mean±sd V'O2 peak·kg-1 % predicted compared with participants without dyspnoea (mMRC 0) (76±16% versus 89±18%; p=0.009) due to higher body mass index (p=0.03). For ICU- versus non-ICU-treated participants, mean±sd V'O2 peak % predicted was 82±15% and 90±17% (p=0.004), respectively. Ventilation, breathing reserve and ventilatory efficiency were similar between the ICU and non-ICU groups.
Conclusions: One-third of participants experienced V'O2 peak <80% predicted 3 months after hospital discharge for COVID-19. Dyspnoeic participants were characterised by lower exercise capacity due to obesity and lower ventilatory efficiency. Ventilation and ventilatory efficiency were similar between ICU- and non-ICU-treated participants.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: I. Skjørten has provided lectures for doctors’ education paid by Norwegian Directorate of Health and Norwegian Medical Association. Conflict of interest: O.A.W. Ankerstjerne has nothing to disclose. Conflict of interest: D. Trebinjac has nothing to disclose. Conflict of interest: E. Brønstad has nothing to disclose. Conflict of interest: Ø. Rasch-Halvorsen has nothing to disclose. Conflict of interest: G. Einvik has received research grants from AstraZeneca and from Boehringer Ingelheim to perform the current study. Conflict of interest: T.V. Lerum has nothing to disclose. Conflict of interest: K. Stavem has nothing to disclose. Conflict of interest: A. Edvardsen is leader of the Norwegian Society for Clinical Physiology (unpaid), and has received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from GlaxoSmithKline and Chiesi. Conflict of interest: C.B. Ingul has received lecture fees from Bayer AS, unrelated to the current study.
Figures
Comment in
-
Phenotyping long COVID.Eur Respir J. 2021 Aug 26;58(2):2101763. doi: 10.1183/13993003.01763-2021. Print 2021 Aug. Eur Respir J. 2021. PMID: 34244323 Free PMC article.
-
Exercise capacity impairment after COVID-19 pneumonia is mainly caused by deconditioning.Eur Respir J. 2021 Dec 31;59(1):2101136. doi: 10.1183/13993003.01136-2021. Print 2022 Jan. Eur Respir J. 2021. PMID: 34737222 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical