

Improving Outpatient Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: A Stepped-Wedge Cluster Randomized Trial
- PMID: 34212177
- PMCID: PMC9630878
- DOI: 10.1093/cid/ciab602
Improving Outpatient Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: A Stepped-Wedge Cluster Randomized Trial
Abstract
Background: Inappropriate antibiotic prescribing is common in primary care (PC), particularly for respiratory tract diagnoses (RTDs). However, the optimal approach for improving prescribing remains unknown.
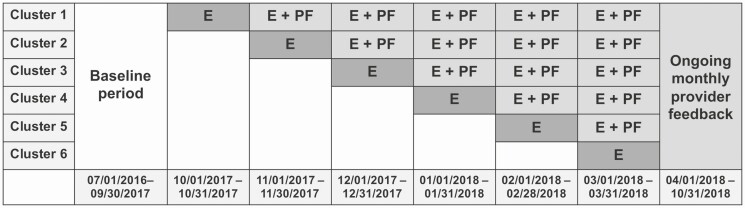
Methods: We conducted a stepped-wedge study in PC practices within a health system to assess the impact of a provider-targeted intervention on antibiotic prescribing for RTDs. RTDs were grouped into tiers based on appropriateness of antibiotic prescribing: tier 1 (almost always indicated), tier 2 (may be indicated), and tier 3 (rarely indicated). Providers received education on appropriate RTD prescribing followed by monthly peer comparison feedback on antibiotic prescribing for (1) all tiers and (2) tier 3 RTDs. A χ 2 test was used to compare the proportion of visits with antibiotic prescriptions before and during the intervention. Mixed-effects multivariable logistic regression analysis was performed to assess the association between the intervention and antibiotic prescribing.
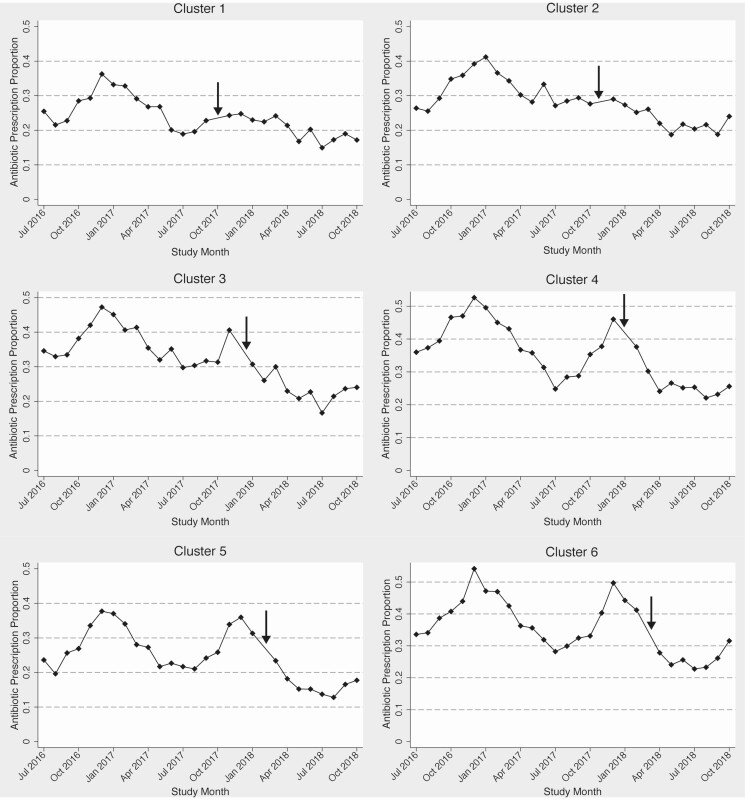
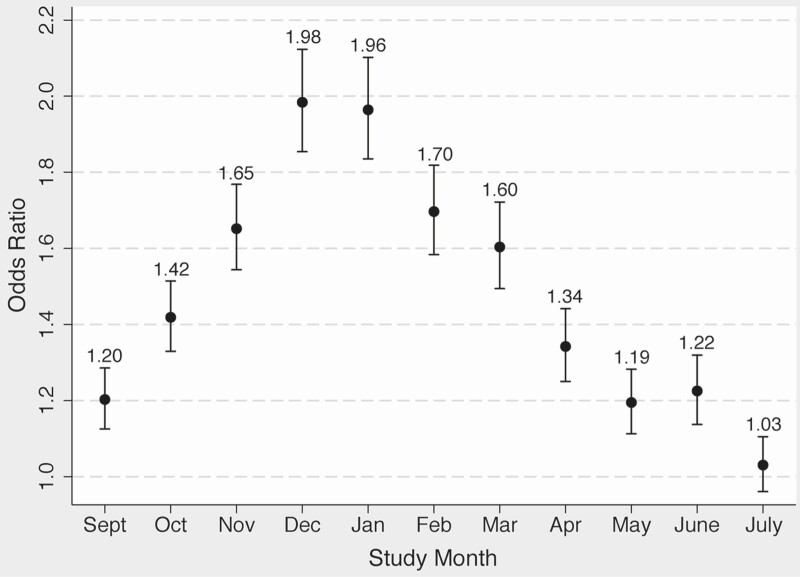
Results: Across 30 PC practices and 185 755 total visits, overall antibiotic prescribing was reduced with the intervention, from 35.2% to 23.0% of visits (P < .001). In multivariable analysis, the intervention was associated with a reduced odds of antibiotic prescription for tiers 2 (odds ratio [OR] 0.57; 95% confidence interval [CI] .52-.62) and 3 (OR 0.57; 95% CI .53-.61) but not for tier 1 (OR 0.98; 95% CI .83-1.16).
Conclusions: A provider-focused intervention reduced overall antibiotic prescribing for RTDs without affecting prescribing for infections that likely require antibiotics. Future research should examine the sustainability of such interventions, potential unintended adverse effects on patient health or satisfaction, and provider perceptions and acceptability.
Keywords: antibiotic prescribing; antibiotic stewardship; antimicrobial stewardship; primary care; respiratory tract infections.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Shapiro DJ, Hicks LA, Pavia AT, Hersh AL. Antibiotic prescribing for adults in ambulatory care in the USA, 2007–09. J Antimicrob Chemother 2014; 69:234–40. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016; 315:1864–73. - PubMed
-
- Deshpande A, Pasupuleti V, Thota P, et al. Community-associated Clostridium difficile infection and antibiotics: a meta-analysis. J Antimicrob Chemother 2013; 68:1951–61. - PubMed
